Cardiovascular diseases in patients with diabetes are common due to metabolic disturbances that accelerate atherosclerosis. These conditions significantly increase the risk of heart attacks, strokes, and vascular complications.
Diabetic patients often develop coronary artery disease at a younger age and with more severe progression. Early detection with imaging and laboratory tests reduces complications and improves treatment outcomes.
Preventive measures, such as strict blood sugar control, lipid management, and lifestyle modifications, are essential in reducing cardiovascular risk in diabetic patients. Personalized care plans are highly effective.
Advanced treatments, including interventional cardiology procedures and modern medications, play a key role in managing cardiovascular disease in diabetes. Regular medical monitoring ensures long-term success.
Why does diabetes damage the heart so much?
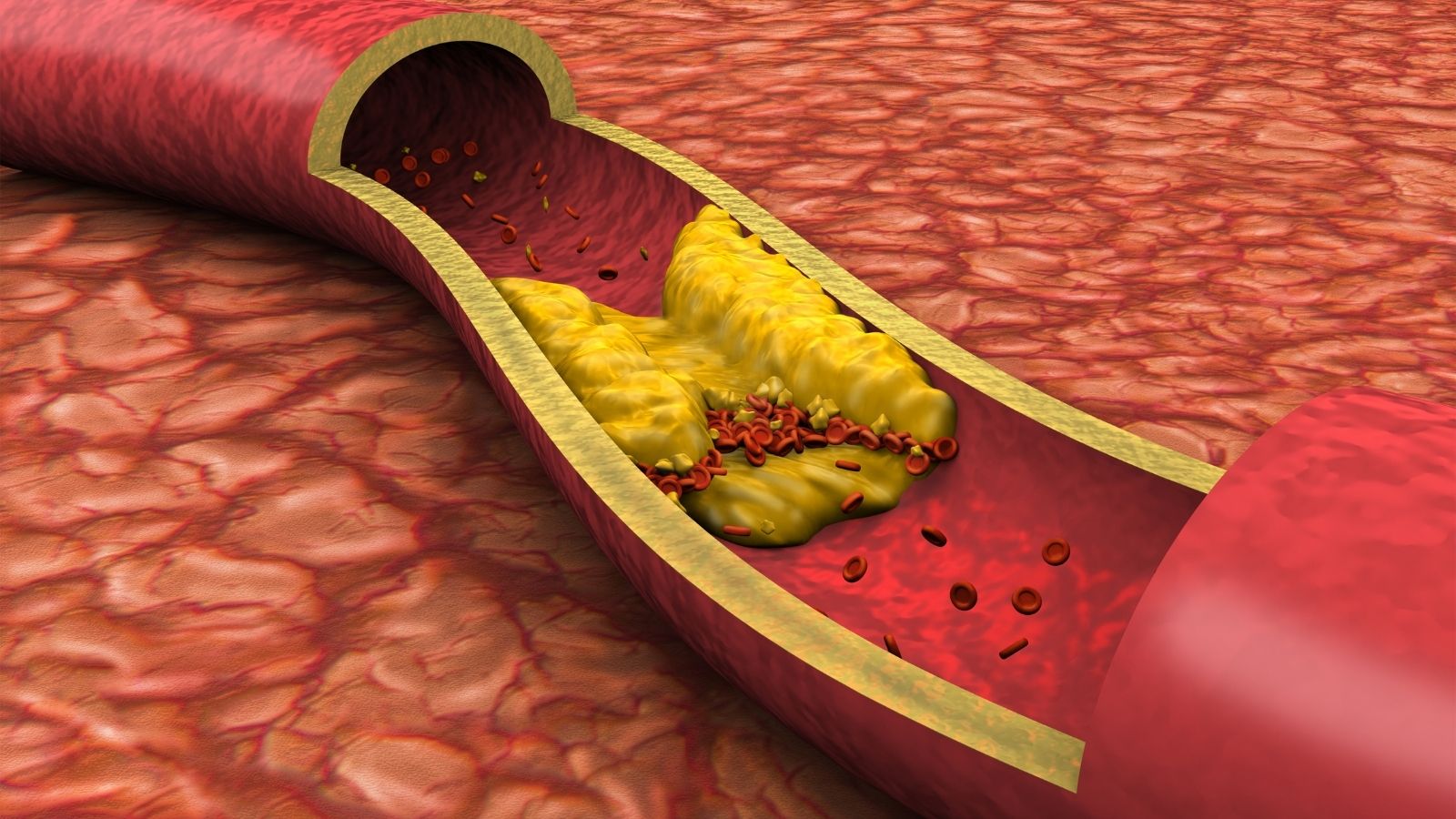
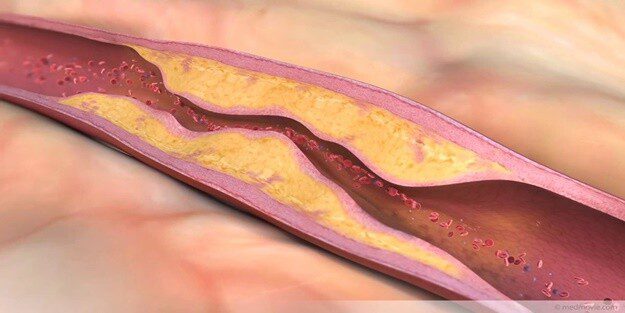
You can think of diabetes as a leak that slowly rots the foundation of a house. It is not noticeable at first, but over time it weakens the whole structure. Diabetes does the same for our blood vessels. High blood sugar levels in our bodies damage the delicate layer that lines the inner surface of the vessels (the endothelium) and protects them. When this protective shield is damaged, the vessels are vulnerable.
This creates a constant state of mild inflammation in the body. This inflammatory environment facilitates the deposition of cholesterol and other fatty substances on the vessel walls. In other words, diabetes both initiates and accelerates the process of atherosclerosis. Therefore, people with diabetes may face cardiovascular problems at a much earlier age than those without diabetes. The vascular age of a young diabetic can be decades older than the calendar age. This explains most clearly why diabetes is considered a “disease accelerator”.
How much does someone with diabetes have an increased risk of heart attack or stroke?
An adult with diabetes is two to four times more likely to have a heart attack or stroke than someone without diabetes. This statistic is one of the clearest indicators of the seriousness of the situation. Moreover, this increased risk can persist not only when blood sugar is high, but even when blood sugar seems to be under control. This is because the negative impact of diabetes on blood vessels is not limited to sugar levels; chronic inflammation, deterioration in blood lipids and other complex mechanisms are also constantly damaging them.
Gender is also a factor affecting this risk. Research shows that women with diabetes may have an even higher risk of developing heart disease than men with diabetes. This indicates that diabetes can have a more aggressive effect on the cardiovascular system of women.
In the past, a diagnosis of Type 2 diabetes was seen as a risk almost equivalent to having had a heart attack before. However, we now know that not all diabetics have the same risk. A young patient with newly diagnosed diabetes is not at the same risk as a patient who has had diabetes for years, smokes and has high blood pressure. Therefore, today’s modern approach requires an individualized assessment of risk and tailoring treatment according to this personal risk profile.
How does high blood sugar destroy blood vessel walls?
High blood sugar levels initiate a rusting process in our blood vessels. This destructive effect proceeds through several interrelated mechanisms.
- Breach of the Protective Shield (Endothelial Damage): The protective layer of cells lining the inside of our blood vessels loses its function when exposed to high sugar. This shield, which ensures the flexibility of the vessels, prevents clotting and regulates blood flow, is disabled. This is the first step to atherosclerosis.
- Accumulation of Harmful Compounds (AGEs): Excess sugar circulating in the blood combines with proteins and fats in the vessel wall to form harmful substances called “Advanced Glycation End Products”. These substances accumulate in the vessel wall and cause the vessels to lose their elasticity and harden. The vessels begin to petrify.
- Increased Cellular Stress (Oxidative Stress): High sugar increases the production of harmful molecules called “free radicals” in our cells. These molecules attack cells and accelerate vascular aging. This cellular stress can target not only the blood vessels but also the heart muscle cells directly, weakening the heart’s pumping power over time.
Why is atherosclerosis more dangerous in patients with diabetes?
Not only does arteriosclerosis progress faster in diabetes, but the structure of the plaques that form also becomes more dangerous. While plaque in someone without diabetes may be more solid and stable, plaque in a patient with diabetes is usually softer, inflamed and “unstable”.
We can liken these unstable plaques to a volcano covered by a thin crust. They can rupture and erupt at any time. When a plaque ruptures, the body recognizes it as a wound and quickly forms a clot on it. This clot can suddenly and completely block the blood vessel, leading to a heart attack or stroke. This means that a P stenosis in a patient with diabetes may be riskier than a P stenosis in someone without diabetes because of the dangerous nature of the plaque.
This “plaque quality” issue explains why we need to be more careful when choosing treatment modalities. Stenting mechanically opens the narrowest spot at the moment, but does not treat the dangerous and inflamed structure of the plaque or the diseased areas beyond and behind the stent. Coronary bypass surgery, on the other hand, bypasses the entire diseased part of the vessel and diverts blood directly to a healthy part of the vessel. This is the main explanation for why bypass surgery offers a more permanent and safer long-term solution, especially in patients with diabetes, in whom vascular disease is common.
what is “diabetic dyslipidemia” and why do you need more than cholesterol medication?
The deterioration of blood lipids in patients with diabetes is much more complex than a simple elevation of “bad cholesterol” (LDL). This condition is called “diabetic dyslipidemia” and poses a much more insidious threat to heart health. The main features of this table are the following:
- High triglyceride levels
- Low levels of “good cholesterol” (HDL)
- The more dangerous “small, dense LDL” particles
The most dangerous of these properties is the change in the structure of LDL cholesterol. LDL particles, which are normally larger, become small and dense in diabetes. These small particles infiltrate the vessel wall much more easily and trigger arteriosclerosis much faster. In other words, even if your LDL cholesterol appears within normal limits in your blood test, if the structure of these particles is impaired, your risk continues. Therefore, it is not enough just to lower cholesterol in patients with diabetes; a comprehensive lifestyle and drug treatment plan that controls triglycerides, raises good cholesterol and corrects this dangerous particle structure is essential.
How insulin resistance and “hidden sugar” initiate heart disease risk
Insulin resistance is the root cause of Type 2 diabetes and starts to damage the heart and blood vessels years before blood sugar starts to rise. When body cells fail to respond properly to insulin, the pancreas secretes more insulin to break this resistance. These excessively high levels of insulin in the blood (hyperinsulinemia) lead to thickening of the vessel walls, increased blood pressure and deterioration of blood fats.
In other words, the risk of heart disease has already started during the period called “prediabetes” (hidden diabetes), before the official diagnosis of diabetes has been made. By the time a patient is diagnosed with Type 2 diabetes, there is usually already a process of damage to the blood vessels that has been going on for about 8-10 years. This fact shows that preventing diabetes actually means preventing heart disease. Intervening during latent diabetes through lifestyle changes is the most effective way to prevent a future heart attack or stroke.
Which cardiovascular diseases are more common in diabetics?
Diabetes can affect the entire vascular system in the body, causing serious problems in different organs. The most common and most dangerous are the following:
- Coronary Artery Disease (CAD)
- Heart Failure
- Stroke (Paralysis)
- Peripheral Arterial Disease (Leg Vascular Occlusion)
Not only are these diseases more common in patients with diabetes, they are also more severe and more difficult to treat. For example, coronary artery disease is often found in many vessels of the heart, rather than in a single vessel. This makes treatment options more complex.
Why can a heart attack be “silent” in patients with diabetes?
One of the most insidious aspects of diabetes is that it damages nerve endings (diabetic neuropathy), reducing the sensation of pain. This can lead to the most typical symptom of a heart attack – chest pain – not being felt. in this so-called “silent heart attack”, the patient may have a serious attack and not realize it. Because it is asymptomatic, the disease progresses, the diagnosis is delayed and unfortunately the first symptom may be sudden death. Therefore, it is vital to check the heart regularly in patients with diabetes, even if there are no obvious complaints.
Is heart failure a hidden consequence of diabetes?
Yes, heart failure is one of the most common but often overlooked complications of diabetes. Heart failure is the inability of the heart to pump enough blood to meet the body’s needs. Even without blockages in the coronary arteries, diabetes can damage the heart muscle directly, disrupting its structure and reducing its pumping power. This condition is called “diabetic cardiomyopathy”.
Interestingly, large studies have shown that heart failure is usually the first cardiovascular problem to occur in patients with Type 2 diabetes. This suggests that heart failure may not be a late consequence of diabetes, but rather an early precursor. These two diseases (diabetes and heart failure) create a vicious circle that feeds each other. Diabetes increases the risk of heart failure, and heart failure increases insulin resistance in the body, making it difficult to control diabetes.
Why is leg vein occlusion important in someone with diabetes?
Peripheral arterial disease (PAD) is a narrowing or blockage of the arteries that most commonly carry blood to the legs. Diabetes is the most important cause of this disease after smoking. The most common symptom is pain or cramping in the legs that occurs with walking and goes away at rest. However, patients with diabetes may not feel this typical pain due to nerve damage. This is why the disease usually progresses insidiously.
Untreated PAH is the leading cause of non-healing foot wounds, infections and ultimately amputation in patients with diabetes. However, it is a big mistake to see PAH as only a leg problem. A blockage in the leg arteries is the strongest sign that the same arteriosclerotic process is probably going on in the arteries supplying the heart and brain. Therefore, a detailed vascular examination of a diabetic patient who complains of pain in their legs or is at risk can not only save their legs but also their life.
Which screening tests and check-ups should be done regularly for heart health?
To protect the heart health of a patient with diabetes, it is essential to be proactive and keep regular check-ups. These checks allow us to catch potential problems at an early stage.
Here are the basic checks that should be done at every doctor’s visit:
- Blood pressure measurement
- Body weight monitoring
- Foot examination
There are also more extensive check-ups that should be done annually or as often as your doctor decides:
A1C Test: It shows your blood glucose average for the last 3 months.
- Blood Fat Profile: Measures your levels of bad (LDL) and good (HDL) cholesterol and triglycerides.
- Ophthalmologic Examination: Checks for damage to the eye vessels caused by diabetes.
- Kidney Function Tests: It assesses your kidney health with urine and blood tests.
If you have symptoms such as shortness of breath, fatigue, pressure in the chest or if your risk profile is high, your doctor may order further cardiac screening tests:
- Electrocardiogram (ECG)
- Echocardiography (Heart ultrasound)
- Effort (Stress) Test
- Cardiac CT Angiography
These tests are not “trouble-shooting” but the most important tools modern medicine has to offer to catch a life-threatening disease that can progress silently, before irreversible damage is done.
What are the most effective lifestyle changes to protect heart health?
Even the most modern medicines or the most successful surgeries alone cannot compensate for the damage caused by an unhealthy lifestyle. Lifestyle changes are the foundation of treatment.
Review Your Dietary Habits
Adopting a heart-friendly diet can have miraculous effects on blood sugar, blood pressure and cholesterol. Plans such as the Mediterranean diet are particularly recommended.
What to avoid or limit:
- Processed meats (salami, sausage, pepperoni)
- Sugary drinks and instant fruit juices
- Packaged products (chips, biscuits, crackers)
- Pastries and white bread
- Foods containing saturated and trans fats (margarine, fast food)
What you should include more of on your table:
- Fresh vegetables in season
- Fibrous fruits
- Whole grain products
- Legumes (chickpeas, lentils, beans)
- Healthy fats (olive oil, avocado, walnuts)
- Lean protein sources (fish, chicken breast)
Aim for at least 150 minutes a week (e.g. 30 minutes 5 days a week) of moderate-intensity exercise, such as brisk walking. Regular exercise allows the body to use insulin more efficiently and supports heart health.
Even as little as a 5-10% reduction in body weight can lead to very significant improvements in your blood sugar, blood pressure and cholesterol levels.
Smoking and diabetes are the deadliest duo for blood vessels. Quitting smoking is the single most important step a diabetic can take to reduce the risk of heart attack and stroke.
What should be the blood pressure and cholesterol targets in diabetics?
In patients with diabetes, these targets are more stringent than in those without diabetes. Because the risk is already higher.
- Blood Pressure (Blood Pressure): The goal for most patients with diabetes is usually below 130/80 mmHg. Achieving this goal usually requires lifestyle changes as well as medication.
- Cholesterol (Blood Fats): Treatment is individualized according to the patient’s overall risk of heart disease. If you have known heart disease or other high risk factors, treatment is much more aggressive. The goal is to lower the level of bad cholesterol (LDL) by more than P, usually below 70 mg/dL, or even below 55 mg/dL in very high-risk cases. Statin drugs are usually used to achieve these goals and other drugs can be added if necessary.
How do new generation diabetes drugs protect the heart?
The last decade has seen revolutionary advances in diabetes treatment. We now have a new generation of drugs that not only lower blood sugar, but also directly protect the heart and blood vessels. These drugs have shifted the focus of diabetes treatment from “just controlling sugar” to “protecting the heart and organs”.
Two main groups of drugs stand out.
- SGLT2 Inhibitors: These drugs lower blood sugar by increasing the excretion of sugar in the urine. But their real miraculous effect is on the heart. They have been shown to significantly reduce hospitalizations and heart-related deaths, especially in patients with heart failure. These drugs have now become a cornerstone of heart failure treatment, whether the patient has diabetes or not.
- GLP-1 Agonists: These drugs work by reducing appetite and regulating insulin release. Their most important benefit is that they have been proven to reduce the incidence of atherosclerosis (heart attack, stroke). They also have the added benefits of providing significant weight loss and lowering blood pressure.
Current treatment guidelines strongly recommend the addition of one of these new generation drugs with proven cardioprotective effects in patients with known heart disease or high-risk diabetes.
Is stent or bypass surgery better for advanced vascular occlusion?
When coronary artery disease progresses despite medication and lifestyle changes, it is necessary to open the blocked vessels to restore blood flow to the heart. There are two main methods for this: Stenting (PCI) and coronary bypass surgery (CABG).
The answer to the question of which method is better, especially for patients with diabetes who have severe stenosis in more than one vessel (multi-vessel disease), is quite clear with scientific evidence. Large and long-term scientific studies have consistently shown that in this patient group, bypass surgery provides superior long-term results compared to stenting.
| Evaluated Result | Stent (PCI) | Bypass Surgery (CABG) |
| Long Term Survival | Lower | Higher |
| Long-term Risk of Heart Attack | Higher | Lower |
| Need for Re-Vascularization | Much Higher | Much Lower |
| Short-Term Stroke Risk | Lower | Higher |
| Recovery Process | Fast and Easy | Slower and More Challenging |
The main reason for this long-term superiority of bypass surgery is that it more radically solves the problem of widespread and “poor quality” plaque in the vessels caused by diabetes. While a stent is a “point repair” that opens the narrowest spot, bypass surgery is a more permanent solution that completely bypasses the diseased vessel area.
Why is a “Heart Team” approach important in treatment decision-making?
In complex situations where diabetes and heart disease coexist, making the right treatment decision can be beyond the expertise of a single physician. For this reason, modern medicine adopts a multidisciplinary approach called “Heart Team”. This team evaluates the patient’s condition from every angle and draws the best treatment path together.
A Heart Team usually includes the following specialists:
- Interventional Cardiologist (physician performing the stent procedure)
- Cardiovascular Surgeon (physician performing bypass surgery)
- Endocrinologist (Diabetes specialist)
- Imaging Cardiologist (physician who interprets tests such as Echo, CT)
- Anesthesiologist

Prof. Dr. Yavuz Beşoğul graduated from Erciyes University Faculty of Medicine in 1989 and completed his specialization in Cardiovascular Surgery in 1996. Between 1997 and 2012, he served at Eskişehir Osmangazi University Faculty of Medicine as Assistant Professor, Associate Professor, and Professor, respectively. Prof. Dr. Beşoğul, one of the pioneers of minimally invasive cardiovascular surgery in Türkiye, has specialized in closed-heart surgeries, underarm heart valve surgery, beating-heart bypass, and peripheral vascular surgery. He worked at Florence Nightingale Kızıltoprak Hospital between 2012–2014, Medicana Çamlıca Hospital between 2014–2017, and İstinye University (Medical Park) Hospital between 2017–2023. With over 100 publications and one book chapter, Prof. Dr. Beşoğul has contributed significantly to the medical literature and is known for his minimally invasive approaches that prioritize patient safety and rapid recovery.