A heart aneurysm is a localized dilatation of the heart wall, often developing after a heart attack. It weakens the cardiac structure and may lead to life-threatening complications.
Symptoms of a heart aneurysm include chest pain, palpitations, shortness of breath, and in some cases, heart failure. Early detection is vital to prevent rupture or arrhythmias.
Treatment options depend on aneurysm size and symptoms, ranging from medication to surgical repair. Surgical intervention is required for large or symptomatic aneurysms.
Long-term monitoring with echocardiography or MRI is essential to track aneurysm progression. Lifestyle modifications and regular cardiology follow-up reduce associated risks.
| Medical Name | Cardiac Aneurysm |
| Frequent Use Areas | – Aneurysms that usually develop in the heart wall after a heart attack – Rarely congenital or trauma-related enlargement of the heart wall |
| Common Symptoms | – Chest pain- Shortness of breath- Rapid fatigue- Heart rhythm disturbances- Sometimes asymptomatic |
| Causes | – Weakening of the heart muscle wall after a heart attack (myocardial infarction) – Congenital connective tissue diseases – Trauma – Infections |
| Risk Factors | – Previous heart attack- Hypertension- Smoking- Family history of aneurysm |
| Complications | – Heart failure – Rhythm disturbances (arrhythmia) – Rupture of the heart wall (rupture) – Clot formation and embolism in the heart |
| Diagnostic Methods | – Echocardiography (ECHO)- Cardiac MRI- CT angiography- Angiography |
| Treatment Methods | – Regular cardiological follow-up – Medication (for heart failure and arrhythmias) – Surgical repair if necessary |
| Prevention Methods | – Reducing the risk of heart attack- Blood pressure and cholesterol control- Healthy lifestyle- Regular cardiology check-ups |
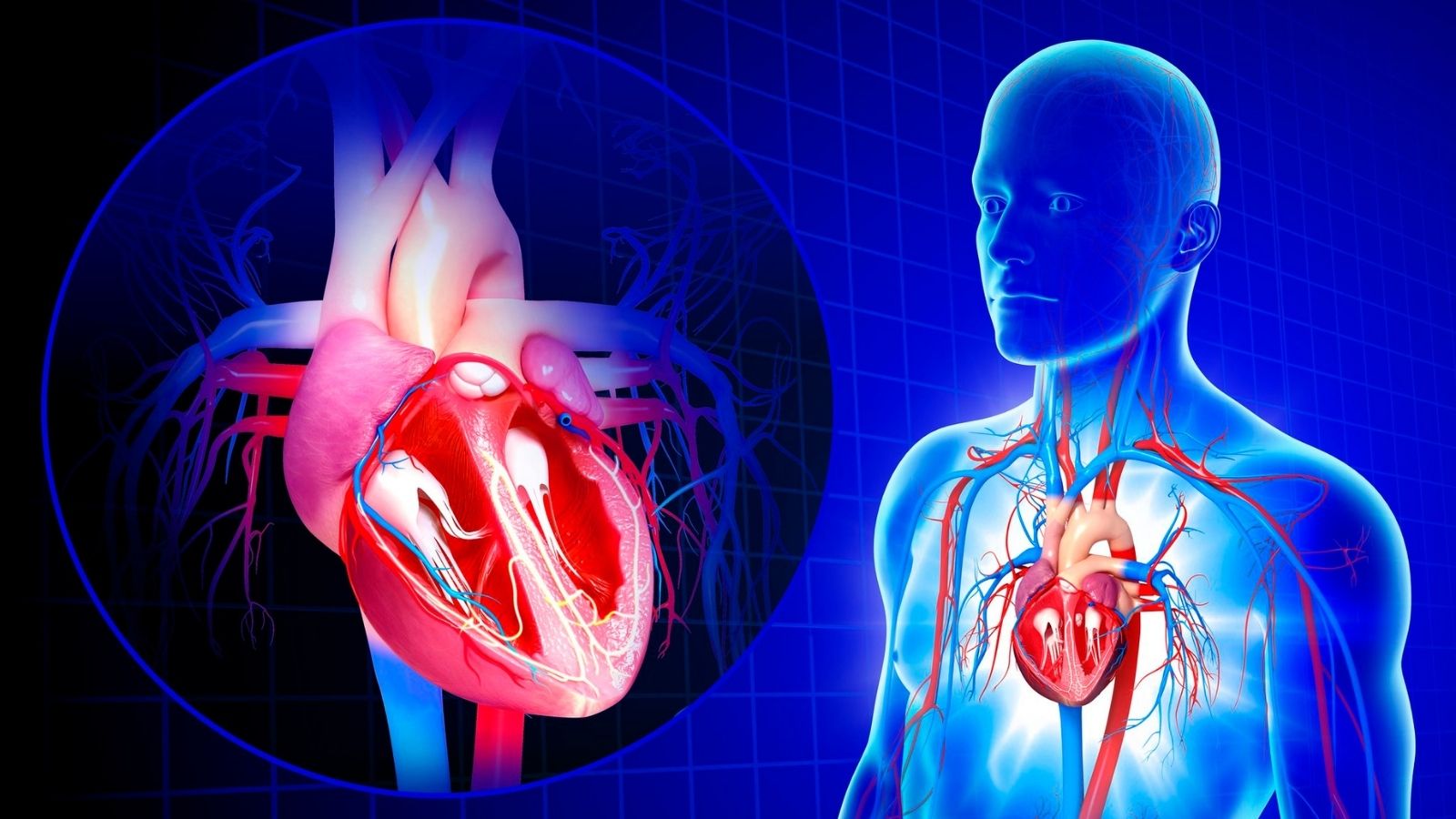
What is a Heart Aneurysm?
The walls of your heart or blood vessels are normally extremely strong and flexible to withstand the high pressure of the blood. However, arteriosclerosis (atherosclerosis), years of high blood pressure, certain genetic diseases or trauma can weaken these walls by destroying their structure. This weakened area cannot withstand the pressure exerted by the blood with each beat of the heart, and over time it stretches outward and widens. For a blood vessel to be medically recognized as an aneurysm, it must be at least one and a half times (P) larger than its normal diameter in that area. This ballooning can occur both directly in the heart’s own muscle tissue (ventricular aneurysm) and in the aorta, the main artery that carries blood from the heart to the entire body (aortic aneurysm).
Why Are Heart Aneurysms Dangerous?
Aneurysms are dangerous because they often grow silently and the biggest fear is that this bubble will suddenly burst. Over time, the wall of an expanding aneurysm becomes thinner and weaker, just as a balloon that is inflated too much increases the risk of bursting. The main dangers of aneurysms are the following:
- Rupture (Rupture)
- Separation of Wall Layers (Dissection)
- Blood Clot Formation (Thrombosis)
Rupture or dissection are conditions that lead to life-threatening internal bleeding and require urgent surgical intervention. Furthermore, clots can form inside the aneurysm sac as blood flow slows down. A piece of these clots can travel through the bloodstream to the brain and cause a stroke, to the heart and cause a heart attack, or to other organs and cause serious damage.
What is the Difference Between Aortic Aneurysm and Ventricular Aneurysm?
the term “heart aneurysm” can refer to two different conditions, and knowing this distinction is important for understanding the nature and treatment of the disease. We can think of an aortic aneurysm as a problem in the body’s main water pipe (plumbing) and a ventricular aneurysm as structural damage directly to the heart engine itself.
An aortic aneurysm forms in the wall of the aorta, the largest artery that exits the heart and distributes blood throughout the body. It is usually caused by general problems affecting the vascular system, such as arteriosclerosis and high blood pressure.
A ventricular aneurysm occurs directly in the wall of the ventricles, the pumping chambers of the heart. In the vast majority of cases, this is caused by weak scar tissue that replaces heart muscle tissue that has died after a previous severe heart attack.
The main points that distinguish these two situations are the following:
Key points for Aortic Aneurysm:
Location: Main Artery (Aorta)
Cause: Arteriosclerosis, High Blood Pressure
Analogy The Body’s Main Plumbing Pipe
Key points for Ventricular Aneurysm:
Location Heart Muscle (Ventricle)
Cause Previous Heart Attack
Analogy Structural Damage to the Heart Motor
What Does True Aneurysm and Pseudoaneurysm Mean?
This distinction is crucial for the risk of an aneurysm and the urgency of treatment. In a true aneurysm, the vessel wall balloons outwards as a whole, retaining its integrity with all its layers. Although the wall has thinned, it is still composed of the vessel’s own layers. This is why mature and hardened true aneurysms have a lower risk of rupture.
A pseudoaneurysm is actually a complete rupture. The heart wall has completely ruptured, but the bleeding is temporarily stopped by the surrounding pericardium or scar tissue. This is like a thin band of tape wrapped around a burst tube. Because its wall does not contain heart muscle, it is extremely fragile. The most critical difference between these two types is their risk of rupture.
True Aneurysm Low Risk of Tearing (After Maturation)
Pseudoaneurysm Very High Risk of Tearing (0-45)
Pseudoaneurysm: Need for Emergency Surgery
Because of this high risk, a false aneurysm diagnosis almost always means emergency surgery.
How Does Aortic Aneurysm Develop and What Causes Cardiovascular Dilation?
The aorta is the largest artery in the body and carries high-pressure blood from the heart to all organs. To withstand this pressure, its walls are multi-layered and strong. However, over the years this robust structure can weaken. The most common cause of cardiovascular dilatation, i.e. aneurysm formation, is arteriosclerosis (atherosclerosis). Fat and limescale (plaques) build up on the vessel walls, causing them to lose their elasticity and weaken. High blood pressure accelerates the process by constantly exerting excessive force on these weakened walls. Smoking also multiplies the risk by directly damaging the vascular wall. Sometimes the problem is genetic. Some connective tissue diseases, such as Marfan syndrome, cause the aortic wall to be congenitally weak, which can predispose to the development of an aortic aneurysm at a young age.
What are the Main Types of Aortic Aneurysm?
Aortic aneurysms are divided into two main types according to their location in the body:
- Abdominal Aortic Aneurysm (AAA)
- Thoracic Aortic Aneurysm (TAA)
AAA is the most common type and occurs in the part of the aorta that runs through the abdomen. TAA is rarer and occurs in the part of the aorta inside the rib cage (where it exits the heart, where it descends along the back or where the vessel arches).
Who is at Risk for Aortic Aneurysm?
Certain factors significantly increase the risk of developing an aortic aneurysm. If you have one or more of these risk factors, it is important to have regular check-ups:
- Smoking (Strongest Risk Factor)
- over 65 Years of Age
- Male Gender
- Family History of Aneurysm
- High Blood Pressure (Hypertension)
- Arteriosclerosis (Atherosclerosis)
- Genetic Connective Tissue Diseases (Marfan Syndrome etc.)
What are the Symptoms of Aortic Aneurysm?
Aortic aneurysms usually grow slowly without causing any symptoms. For this reason, they are also called “silent killers” and are often detected by chance during an abdominal ultrasound or CT scan performed for another reason. When the aneurysm is large enough, it can cause symptoms depending on its location.
Symptoms of an aortic aneurysm in the abdomen may include
- Deep, persistent pain in the abdomen or back
- A pulse sensation around the belly button, like feeling your heart beating
Symptoms of thoracic aortic aneurysm are as follows:
- Pain in the chest or upper back
- Persistent and unexplained cough
- Hoarseness (as a result of pressure on the nerve to the vocal cords)
- Difficulty breathing or swallowing (as a result of pressure on the trachea or esophagus)
How is Aortic Aneurysm Diagnosed and Why is Screening Important?
Because aneurysms are often asymptomatic, screening, especially for those at risk, can save lives. Organizations such as the US Preventive Services Task Force recommend that all men aged 65-75 with a history of smoking should be screened with an abdominal ultrasound at least once in their lifetime. This simple, painless and inexpensive test can catch a potentially fatal aneurysm in its early stages. The main imaging methods used for diagnosis are as follows:
- Ultrasound (especially for screening)
- Echocardiography (ECHO)
- Computed Tomography (CT)
- Magnetic Resonance (MR) Imaging
Among these tests, CT is the method that shows the size, location and shape of the aneurysm in the most detail and is considered the gold standard for surgical planning.
Why Does a Heart Bubble Occur and How Does a Ventricular Aneurysm Form?
The most common answer to the question “what causes a bubble in the heart” is a major heart attack. During a heart attack, when one of the coronary arteries supplying the heart is blocked, the area of the heart muscle supplied by that artery is starved of blood and dies. The body removes this dead muscle tissue and replaces it with a flexible scar that is incapable of contracting. While healthy heart muscle pumps blood forward every time it contracts, this weak scar tissue cannot resist the high pressure inside and bulges outwards like a balloon. Over time, this swelling becomes permanent and a structure called a ventricular aneurysm forms.
What Are the Risk Factors for Ventricular Aneurysm?
There are certain conditions that increase the risk of developing an aneurysm after a heart attack. How severe the heart attack is and how quickly it is responded to are the most important factors determining whether this long-term complication will develop:
- Complete blockage of the vessel supplying the anterior wall of the heart (LAD)
- Failure to open the blocked vessel in time with methods such as angioplasty
- Insufficient alternative blood vessels (collaterals)
- A major heart attack affecting all layers of the heart wall (Transmural MI)
What are the Symptoms of Ventricular Heart Aneurysm?
Small aneurysms can be asymptomatic for years. But as the aneurysm grows, it reduces the overall pumping power of the heart, leading to heart failure, which is a major cause of cardiovascular disease. When symptoms appear, they are usually symptoms of heart failure and include
- Shortness of breath (especially with exertion or when lying down at night)
- Constant fatigue and weakness
- Swelling in the ankles and legs (edema)
- Chest pain (angina)
- Palpitations (arrhythmia)
What are the Possible Complications of Ventricular Aneurysm?
These are the serious problems that a ventricular aneurysm can cause: These complications can severely reduce the patient’s quality of life and can be life-threatening:
- Progressive Heart Failure
- Blood Clots and Risk of Stroke (Thromboembolism)
- Life-threatening Rhythm Disorders (Ventricular Arrhythmias)
One of the most dangerous consequences is a clot in the aneurysm sac that can be thrown into the brain and cause permanent strokes. The border zone between scar tissue and healthy muscle tissue can be a source of dangerous rhythm disturbances.
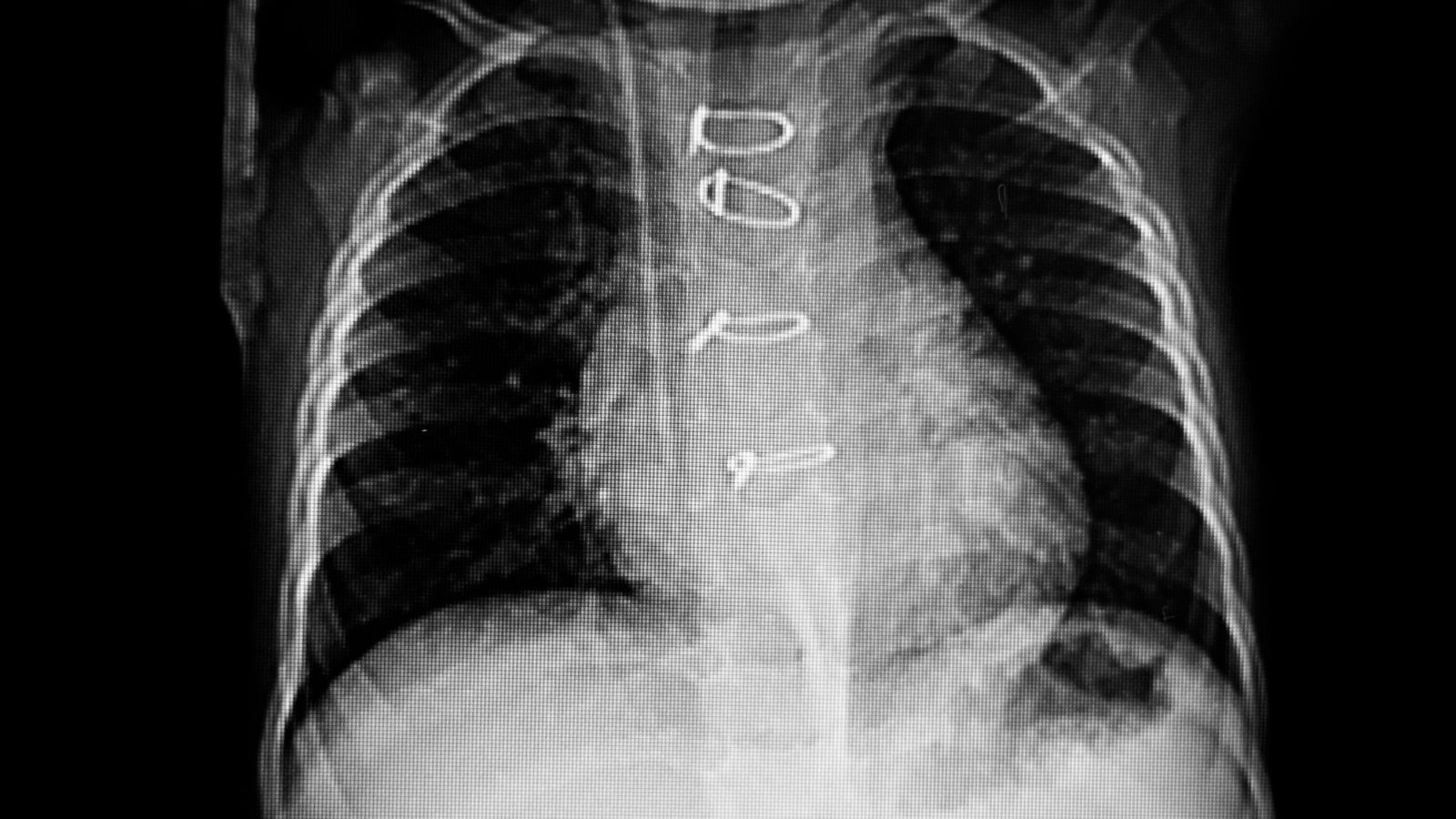
Which Tests are Used in the Diagnosis of Ventricular Aneurysm?
Various tests are used to confirm the diagnosis. These tests are performed to confirm the presence of an aneurysm, measure its size, assess its impact on heart function and detect a possible clot:
- Electrocardiogram (ECG)
- Chest X-ray
- Echocardiography (ECHO) (The most important diagnostic tool)
- Cardiac MRI
- Heart Catheterization (Angiography)
Among these tests, ECHO plays a key role as it can directly visualize the aneurysm, check for the presence of clots and measure the pumping power of the heart (ejection fraction).
Is Heart Aneurysm Treatment Necessary for Every Aneurysm?
No, not all aneurysms require emergency surgery. Especially in small, slow-growing and asymptomatic aneurysms, the risks of surgery itself may be greater than the risk of the aneurysm itself. In these cases, a strategy called “watchful waiting” is followed. This does not mean that the patient is left alone. Rather, it is an active process in which the patient is monitored much more closely and risk factors are aggressively controlled. Non-surgical management includes the following key elements:
- Medicines for blood pressure control
- Cholesterol-lowering drugs (Statins)
- Blood thinners (especially against the risk of clots in ventricular aneurysms)
- Absolute cessation of smoking
- Follow-up with regular imaging (every 6-12 months)
When Is Aortic Aneurysm Surgery Decided?
The decision to operate is made when the risk of rupture of the aneurysm is higher than the risks of surgery. This decision depends on many factors, such as the size of the aneurysm, its rate of growth, the patient’s general health and the presence of symptoms. Surgical intervention usually becomes necessary in the following cases:
- Reaching a certain diameter (usually 5.5 cm for the abdomen, 5-6 cm for the chest)
- Rapid growth (more than 1 cm per year)
- The appearance of symptoms such as pain
- Tearing or dissection (Emergency)
How is Open and Endovascular (EVAR/TEVAR) Aortic Aneurysm Surgery Performed?
There are two main surgical approaches for aortic aneurysm. Open surgery is the traditional approach. A large incision is made in the abdomen or chest wall to access the aneurysm directly. The damaged part is removed and replaced with a sturdy tube (graft) made of a synthetic material such as Dakron. This is a major surgery that is highly effective but has a longer recovery period.
Endovascular repair (EVAR/TEVAR) is a more modern and minimally invasive method. Through a small incision in the groin, a thin tube called a catheter is inserted into the aneurysm. Through this catheter, a fabric-covered metal stent (stent-graft) is inserted into the aneurysm. When the stent-graft opens, it creates a new pathway for blood flow and protects the aneurysm sac from pressure and disables it. The advantage of this method is a smaller incision, less pain and a much faster recovery time. However, the vascular anatomy of each patient may not be suitable for this method.
When is Ventricular Aneurysm Surgery Decided?
Ventricular aneurysm surgery is considered when serious problems arise that impair the patient’s quality of life or threaten his or her life despite medication. The decision to operate is usually taken in severe cases that do not respond to medication:
- Symptoms of progressive heart failure
- Uncontrolled chest pain
- Dangerous rhythm disturbances
- History of clotting (embolism)
What is Left Ventricular Reconstruction and Dor Procedure?
The goal of ventricular aneurysm surgery is not only to remove the damaged tissue but also to improve the pumping function of the heart by correcting its distorted geometry. In this surgery, called Left Ventricular Reconstruction (LVR), the non-contractile scar tissue (aneurysm) is removed and the remaining healthy parts of the heart are reconnected to make the heart work more efficiently.
The Dor Procedure is a more refined and specialized technique of this reconstruction. The aim is to restore the inefficient, spherical heart shape caused by the heart attack to the original, more efficient conical/elliptical shape of the heart. The surgeon separates the dysfunctional area from the heart cavity by placing a circular suture at the base of the aneurysm, usually using a patch. This is not just a repair but an engineering solution to improve the mechanical efficiency of the heart and is usually performed in combination with coronary bypass surgery.
What is the Recovery Process After Aneurysm Surgery?
Postoperative recovery depends on the type of surgery performed. After open surgery, patients stay in intensive care for a few days and are hospitalized for a week in total. It may take 2-3 months to return to normal life completely. With endovascular (closed) methods, these periods are much shorter. There are some restrictions to be aware of in the first weeks of recovery:
- Not driving (usually 4-6 weeks)
- No heavy lifting (more than 5 kg)
- Avoiding strenuous exercise
- Careful wound care
How Long Does Aortic Disease Last and What Are the Long-Term Outcomes?
This is one of the most frequently asked questions by patients and their relatives. A successful aneurysm surgery is not an end but a new beginning for a healthy life. Long-term life expectancy after both aortic aneurysm and ventricular aneurysm repair is quite good and many patients reach their normal life expectancy. However, this depends to a large extent on how well the patient adapts to postoperative lifestyle changes, whether he or she quits smoking and keeps other risk factors such as blood pressure under control. With successful surgery and good medical follow-up, patients’ quality of life and life expectancy are significantly improved.
Which Lifestyle Changes Are Important After Surgery?
Surgery solves the mechanical problem but does not eliminate the underlying vascular disease. These are therefore the most important lifestyle changes you need to make for long-term success:
- Quit smoking completely and definitely
- Heart-friendly diet (low in salt, saturated fat and processed foods)
- Keeping blood pressure under control at ideal levels
- Learning stress management techniques
- Regular and moderate physical activity approved by your doctor (walking, swimming, etc.)
What Is Cardiac Rehabilitation and How Does It Help Recovery?
Cardiac rehabilitation is a comprehensive, medically supervised program designed to speed recovery from heart surgery or a heart attack and prevent future heart problems. This program is not just about exercise. It includes exercise training, education on heart health and nutrition, counseling and psychological support. Cardiac rehabilitation is scientifically proven to reduce the risk of death and improve quality of life. It is one of the most important parts of your recovery and is highly recommended.

Prof. Dr. Yavuz Beşoğul graduated from Erciyes University Faculty of Medicine in 1989 and completed his specialization in Cardiovascular Surgery in 1996. Between 1997 and 2012, he served at Eskişehir Osmangazi University Faculty of Medicine as Assistant Professor, Associate Professor, and Professor, respectively. Prof. Dr. Beşoğul, one of the pioneers of minimally invasive cardiovascular surgery in Türkiye, has specialized in closed-heart surgeries, underarm heart valve surgery, beating-heart bypass, and peripheral vascular surgery. He worked at Florence Nightingale Kızıltoprak Hospital between 2012–2014, Medicana Çamlıca Hospital between 2014–2017, and İstinye University (Medical Park) Hospital between 2017–2023. With over 100 publications and one book chapter, Prof. Dr. Beşoğul has contributed significantly to the medical literature and is known for his minimally invasive approaches that prioritize patient safety and rapid recovery.