Aortic insufficiency treatment focuses on relieving symptoms and preventing heart failure. It is a condition where the aortic valve does not close properly, causing blood to leak back into the left ventricle.
Medical therapy includes vasodilators and diuretics to reduce cardiac workload. Regular echocardiographic monitoring is essential to evaluate progression and determine surgical timing.
Surgical intervention involves aortic valve repair or replacement. The decision depends on the severity of regurgitation, ventricular function, and patient-specific risk factors.
Long-term management includes blood pressure control, endocarditis prophylaxis, and cardiology follow-up. Lifelong care ensures better outcomes and reduces the risk of recurrent complications.
|
Causes |
Degenerative valve disease, bicuspid aortic valve, rheumatic disease, endocarditis, aortic root dilatation (e.g. Marfan syndrome), trauma |
|
Risk Factors |
Hypertension, connective tissue diseases (Marfan, Ehlers-Danlos), advanced age, previous infections |
|
Symptoms |
Shortness of breath, fatigue, palpitations, chest pain, fainting, wide pulse pressure that increases with exercise |
|
Diagnostic Methods |
Diastolic murmur on physical examination, transthoracic/transesophageal ECHO, CT/MR aortic imaging, cardiac catheterization |
|
Treatment Options |
Medical treatment (ACE inhibitors, diuretics), regular follow-up (in asymptomatic patients), surgical aortic valve replacement or TAVI |
|
Complications |
Left ventricular dilatation, left heart failure, arrhythmia, sudden cardiac death |
|
Protective Measures |
Control of hypertension, follow-up of connective tissue diseases, prevention of infections, regular ECHO monitoring |
What is Aortic Valve Failure?
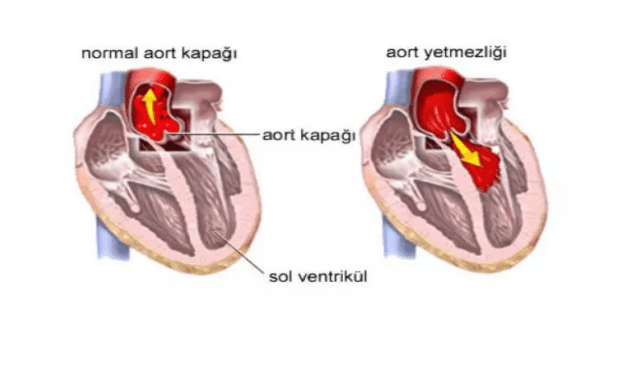
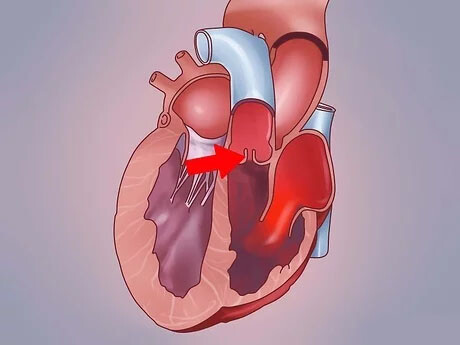
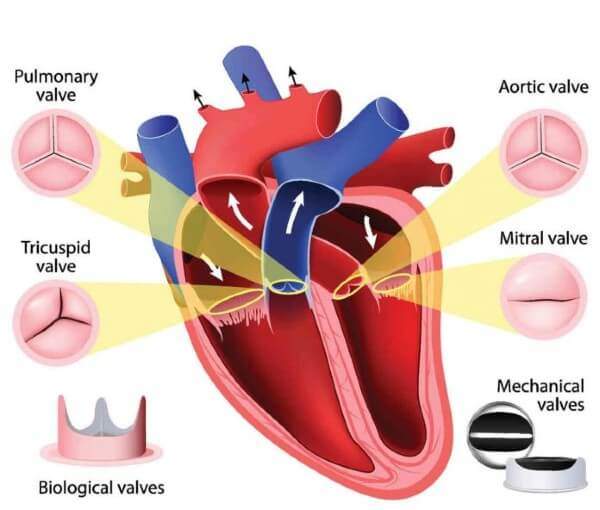
Our heart is an amazing organ that works tirelessly to pump blood continuously throughout our body. It has four valves to ensure that this pumping happens perfectly, so that blood always flows in one direction. One of these valves, the aortic valve, acts as a gateway between the left ventricle, the heart’s most powerful contractile chamber, and the aorta, the body’s largest artery. In a healthy heart, this valve opens wide when the heart contracts, allowing clean blood to be pumped throughout the body, and closes tightly when the heart relaxes, preventing blood from escaping back into the heart.
Aortic insufficiency, also known as aortic valve insufficiency, is a condition in which this aortic valve fails to close. When the valve does not close properly, some of the blood that should be sent to the body leaks backwards into the left ventricle with each relaxation of the heart. This means an unexpected additional workload for your heart. This is because the left ventricle has to pump both normal blood from the lungs and extra blood leaking back through the aorta in the next contraction.
To adapt to this overtime, the heart muscle changes over time. The left ventricle enlarges (dilates) to accommodate the increased blood volume and its walls thicken (hypertrophy) to handle the extra load. Initially, these changes are an adaptation mechanism that helps your heart to maintain its function. This is why many people with chronic aortic insufficiency can live for years without symptoms, without suspecting anything. However, this is not something the heart can tolerate forever. Over time, the heart muscle becomes tired and weak and this can lead to more serious problems such as heart failure.
There is also an “acute” form of the disease that comes on suddenly and worsens rapidly. In this case, the heart does not have time to adapt to this sudden and massive blood leakage and a much more serious condition occurs, requiring urgent intervention.
What are the Symptoms of Aortic Valve Failure?
Aortic insufficiency is often an insidious disease. In particular, people with mild aortic insufficiency, or grade 1 aortic insufficiency as it is medically referred to, may not show any symptoms for years. Often the disease is detected by chance during a medical examination or echocardiography for another reason. But as the disease progresses and the heart’s workload increases, your body starts to give you signals.
The most common symptoms are:
Shortness of breath Perhaps the most common and most important symptom. Initially, it occurs only in situations that require effort, such as climbing stairs or brisk walking. As the disease progresses, you may feel short of breath while walking in a straight line or even at rest. Waking up with sudden shortness of breath some time after going to bed at night, or not being able to lie flat and needing to increase the number of pillows, may indicate that the condition has become serious.
Fatigue and weakness: You may feel tired and fatigued, especially at the end of the day or when you are a little more active than usual, which is not easily relieved by rest. This is an indication that your heart is struggling to keep up with the body’s increased oxygen demand.
Palpitations You may feel your heart beating faster, stronger or irregularly. Patients often describe this sensation as “a bird fluttering in my chest” or “my heart feels like it is going to jump out of my chest”.
Chest pain or discomfort: Due to the increased workload and oxygen demand of the heart muscle, angina-type pain may occur, which manifests itself as pressure, tightness or pain in the chest, especially during exertion. Sometimes these pains can also occur at night.
Swelling of the ankles and legs (edema): When heart failure begins to develop, the body begins to retain fluid, most commonly in the ankles and legs.
Dizziness and fainting: In advanced stages of the disease, insufficient blood supply to the brain can lead to dizziness, blackouts and even sudden fainting (syncope).
If you have early signs of grade 1 aortic insufficiency or any of the above-mentioned symptoms, the most important step for early diagnosis is not to attribute them to “aging” or “fatigue” but to consult a cardiologist.
What Causes Aortic Insufficiency?
Aortic insufficiency can be caused by a congenital problem or by a variety of acquired diseases. Basically, two mechanisms are involved: either the valve leaflets themselves deteriorate, or the root of the aortic vessel in which the valve sits expands and prevents the valves from touching each other.
Congenital Causes:
Bicuspid Aortic Valve: The most common congenital cause. The aortic valve, which normally has three leaflets, is congenitally bicuspid in some people. This causes the valve to wear out earlier, calcify and fail to close completely, paving the way for aortic insufficiency in young and middle age.
Subsequent (Acquired) Causes:
Age-related Degeneration: With advancing age, calcification and hardening of the valve leaflets may occur. Although this condition usually leads to aortic stenosis, it can also cause insufficiency by impairing the elasticity of the valve.
Rheumatic Fever Rheumatic fever triggered by inadequately treated beta-streptococcal throat infections in childhood can cause permanent damage to the heart valves. This is an important cause of aortic insufficiency, especially in developing countries.
Infective Endocarditis: Infection of the heart valves. When bacteria settle in a damaged heart valve through the bloodstream, they can cause perforations and tears in the valve structure, leading to sudden (acute) and severe aortic insufficiency.
Enlargement of the aortic root (aortic aneurysm): The enlargement of the part of the aorta where the aortic artery exits the heart for various reasons (uncontrolled high blood pressure, aging, genetic connective tissue diseases, etc.) pushes the valve leaflets away from each other. Even if the leaflets are healthy, because of this enlargement they cannot touch each other and close completely and leakage begins.
Connective Tissue Diseases: Genetic diseases such as Marfan syndrome and Loeys-Dietz syndrome weaken the structure of the aortic vessel wall, leading to dilatation and thus aortic insufficiency.
Aortic Dissection: It is a rupture of the aortic vessel wall. This is an emergency condition that can disrupt the support of the aortic valve and cause sudden and life-threatening aortic insufficiency.
High Blood Pressure (Hypertension): Uncontrolled high blood pressure over many years can put constant pressure on the aortic artery, contributing to its enlargement and impaired valve function.
How is Aortic Insufficiency Diagnosed?
The diagnosis of aortic insufficiency is a process that usually starts with listening to the patient’s complaints and is confirmed by various technological tests.
Physical Examination: After questioning your medical history and symptoms, your doctor listens to your heart with a stethoscope. In aortic regurgitation, an abnormal sound called a typical “murmur” is heard as blood leaks back during the relaxation phase of the heart. This murmur is an important clue for diagnosis. Changes in your pulse rate and blood pressure can also be instructive.
Echocardiography (ECHO): This test is considered the “gold standard” in the diagnosis of aortic regurgitation. It is an ultrasound procedure that uses sound waves to produce moving images of your heart and valves. It is painless and harmless. With ECHO
The structure of the aortic valve (e.g. whether it is bicuspid or not) is clearly visible.
Precisely measure how much leakage there is in the valve (degree of insufficiency: mild, moderate, severe).
It is assessed how much your heart is enlarged by this leak (left ventricular size) and whether its contractility (ejection fraction – LVEF) is affected.
The aorta is checked for dilatation.
Other Tests: Further tests such as electrocardiogram (ECG), chest x-ray, cardiac magnetic resonance imaging (MRI), computed tomography (CT) or cardiac catheterization may be used to obtain additional information if necessary. Coronary angiography is a standard approach to check the condition of the coronary vessels supplying the heart, especially in patients who are scheduled for surgery.
1,2,3-4 Degree Aortic Valve Insufficiency
Aortic insufficiency grades indicate the amount of blood leakage that occurs when the valves of the aorta, the main artery leaving the heart, fail to close properly. These grades are important for determining the severity of the disease and the need for treatment.
- Grade Aortic Valve Insufficiency (Mild/Minimal): There is mild aortic valve leakage. Patients usually have no significant complaints. It is followed up with routine control and echocardiography.
- Grade Aortic Valve Insufficiency (Moderate): Blood leakage becomes more pronounced. The patient may tire quickly even during light exertion, but daily activities are usually not affected. It is followed up with regular echocardiography and physical examination. More frequent follow-up is recommended as there is a risk of progression.
- Grade Aortic Valve Insufficiency (Intermediate to Advanced): Leakage is at serious levels. The left heart chambers may start to enlarge and the workload of the heart increases. Symptoms such as palpitations, shortness of breath and weakness become prominent. Cardiologic evaluation should be performed more frequently and surgical options should be considered.
- Grade Aortic Valve Insufficiency (Advanced): There is a very serious level of blood leakage. Significant enlargement of the heart chambers and heart failure may develop. The patient may experience complaints even at rest; shortness of breath, chest pain and severe fatigue occur. Surgical intervention, valve repair or replacement is usually unavoidable.
This grading is based on echocardiography results and plays a critical role in the patient’s treatment.
How is Aortic Valve Failure Treated?
The treatment of aortic insufficiency is not based on a “one size fits all” approach. The treatment plan is individually tailored to the severity of the disease, whether you have symptoms, how much your heart is affected and your general health.
Follow-up and Observation: In the early stages, such as mild aortic insufficiency or grade 1-2 aortic insufficiency, if you have no symptoms and your heart function is normal, no emergency treatment is usually started. Instead, you will be closely monitored at regular intervals (usually every 6 months or year) with a doctor and echocardiography. 1.treatment for grade aortic insufficiency usually consists of this follow-up period. The aim is to detect disease progression early.
Drug Therapy: If the patient is hypertensive, they can be used to relieve symptoms, control high blood pressure and slow the development of heart failure by reducing the workload on the heart. However, in hypotensive and weak patients, these drugs increase symptoms and palpitations.
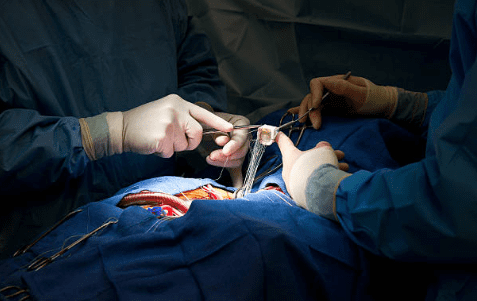
Surgical Treatment: When aortic insufficiency progresses, that is, when it becomes severe, causes symptoms, or when echocardiography reveals impaired cardiac function (decreased contractile strength) or excessive enlargement of the heart even in the absence of symptoms, the definitive treatment is surgery. The aim of surgical intervention is to solve the problem before irreversible damage to the heart occurs and to restore the patient to normal life expectancy and quality.
Aortic Valve Insufficiency Surgery Options
A single method should not come to mind when we think of aortic valve surgery. With the development of technology and surgical techniques, there are different options that offer the most suitable solution for each patient.
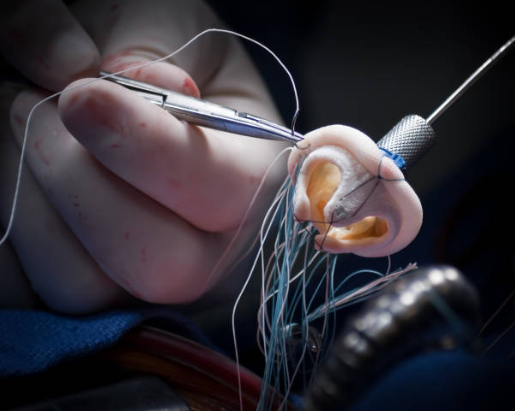
Aortic Valve Repair: Whenever possible, the first preferred method is to preserve and repair the patient’s own valve. If the cover leaflets are not excessively calcified or damaged, the cover can be resealed with various special stitching and reshaping techniques.
Advantages: The biggest advantage is that your body’s own tissue is preserved. This eliminates the need for lifelong use of blood thinners (anticoagulants). There is also a lower risk of infection and the heart’s function is better preserved.
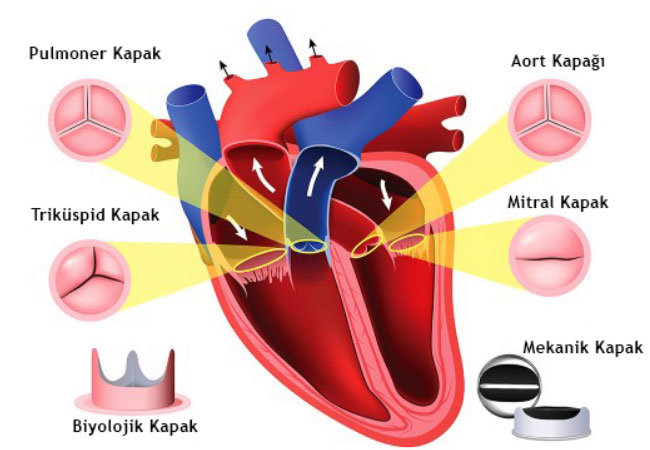
Aortic Valve Replacement: If the valve is damaged beyond repair, the diseased valve is removed and replaced with an artificial valve. There are two main types of artificial cover:
Mechanical Covers: They are made of very durable materials such as carbon and usually last a lifetime. Therefore, they are preferred in younger patients. However, in order to prevent the formation of clots on their surface, the patient must take blood thinners (Warfarin) for life and be monitored with regular blood tests (INR).
Biological (Bioprosthetic) Valves: They are usually made from specially treated bovine or porcine heart tissue. Their biggest advantage is that they usually do not require lifelong blood thinners. However, they are not as long-lasting as mechanical valves; they can wear out in an average of 10-20 years and may require reoperation. Therefore, they are preferred in older patients.
Minimally Invasive Surgery: While the sternum is completely opened in traditional open heart surgery, a very old technique in minimally invasive surgery can be performed with much smaller incisions by opening the side of the chest or only a small part of the sternum. However, the most successful and undamaged technique today is aortic valve repair or replacement, which is performed through a 4-5 cm incision in the armpit and between the ribs without cutting any bone or muscle. This approach offers significant advantages such as less pain, faster recovery, shorter hospitalization and better cosmetic results.
TAVI (Transcatheter Aortic Valve Implantation): TAVI, also known as non-surgical valve replacement, is a method in which the aortic valve is replaced by inserting a catheter through the groin vein. However, TAVI was mainly developed for aortic stenosis due to calcification. In pure aortic insufficiency, the use of standard TAVI devices is limited because there is no calcareous ground for the valve to adhere to. Although new technologies are being developed in this area, surgery is currently the standard treatment for aortic insufficiency. TAVI has almost no chance of success. It can only be considered as an option in selected elderly, special cases where the risk of surgery is very high.
Does Untreated Mild Aortic Insufficiency Progress? Will it kill you?
This is one of the questions that patients and their relatives are most curious and concerned about. The answer is clear: Yes, severe and untreated aortic insufficiency can be life-threatening and lead to serious fatal consequences.
The heart tries to compensate for this additional load for a long time. At some point, however, these compensation mechanisms become inadequate and serious complications arise:
Heart Failure: The most common outcome. The heart can no longer pump enough blood to meet the body’s needs.
Heart Rhythm Disorders (Arrhythmias): The enlarged and deconstructed heart can lose its normal electrical rhythm. This can lead to serious rhythm problems that increase the risk of stroke.
Infective Endocarditis: The damaged valve becomes more vulnerable to infections.
Sudden Cardiac Death: Although rare, there is a risk of sudden cardiac arrest due to fatal rhythm disturbances, especially in advanced, symptomatic and untreated patients.
However, the most important point to emphasize here is this: This unfavorable picture is only valid if the disease is left to its own course. Thanks to modern diagnosis and treatment methods, the vast majority of patients who present on time and receive the right treatment can lead a healthy and normal life without experiencing these complications. Early diagnosis and timely surgical intervention can halt the progression of the disease and normalize life expectancy.
How Should People with Aortic Insufficiency Live?
Being diagnosed with aortic insufficiency or undergoing valve surgery is not the end of life; on the contrary, it means becoming a healthy person because the malfunctioning heart valve is replaced with a heart valve that opens and closes regularly. in 1 month they can perform daily activities and in 6 months they can perform advanced exercises.
It is important for him/her to live as a normal person in the future. It is important to take prophylactic antibiotics to prevent infection in case of dental infection or intravenous interventions and not to neglect blood thinners
Frequently Asked Questions
What is aortic insufficiency?
It is a valve disease in which blood from the heart escapes back into the heart due to incomplete closure of the aortic valve.
Why does it happen?
There can be many causes, such as rheumatic diseases, bicuspid aortic valve, aortic aneurysm, infections (endocarditis) and connective tissue diseases.
What are the symptoms?
Palpitations, shortness of breath, chest pain, rapid fatigue and swelling of the ankles may occur in the later stages.
Is aortic insufficiency dangerous?
Yes, left untreated, the heart muscle gets tired and heart failure can develop.
In which age group is it more common?
It is more common in middle-aged and older individuals; however, it can also occur in young people due to some congenital causes.
How is it diagnosed?
Echocardiography (ECHO) can clearly visualize a leak in the aortic valve.
Is aortic insufficiency progressive?
Yes, over time it can reduce the pumping power of the heart and the disease can worsen.
Is drug treatment enough?
In mild cases, medication can reduce the heart load, but in severe cases surgery may be needed.
How is surgical treatment performed?
Aortic valve repair or valve replacement (with a mechanical or biological valve).
When is surgery necessary?
Surgery is recommended when heart enlargement, symptom development or valve insufficiency becomes severe.
Does life expectancy increase after valve replacement?
Yes, symptoms are reduced, heart function is preserved and life can be prolonged.
Should mechanical or biological valve be preferred?
Mechanical valves are generally preferred in young patients and biological valves in the elderly.
Can I exercise?
In mild and moderate cases, controlled exercise can be done; in severe insufficiency, medical supervision is essential.
Is aortic insufficiency genetic?
Some cases may be genetic (e.g. Marfan syndrome), but most of the time they develop due to age or disease.

Prof. Dr. Yavuz Beşoğul graduated from Erciyes University Faculty of Medicine in 1989 and completed his specialization in Cardiovascular Surgery in 1996. Between 1997 and 2012, he served at Eskişehir Osmangazi University Faculty of Medicine as Assistant Professor, Associate Professor, and Professor, respectively. Prof. Dr. Beşoğul, one of the pioneers of minimally invasive cardiovascular surgery in Türkiye, has specialized in closed-heart surgeries, underarm heart valve surgery, beating-heart bypass, and peripheral vascular surgery. He worked at Florence Nightingale Kızıltoprak Hospital between 2012–2014, Medicana Çamlıca Hospital between 2014–2017, and İstinye University (Medical Park) Hospital between 2017–2023. With over 100 publications and one book chapter, Prof. Dr. Beşoğul has contributed significantly to the medical literature and is known for his minimally invasive approaches that prioritize patient safety and rapid recovery.