Rheumatic heart disease is a complication of untreated streptococcal throat infections, leading to inflammation and permanent damage of the heart valves. The immune response mistakenly attacks cardiac tissue, causing long-term dysfunction.
Symptoms of rheumatic heart disease include fever, joint pain, skin rash, and shortness of breath. Over time, valve scarring may lead to murmurs, fatigue, palpitations, and progression toward heart failure if not managed properly.
Diagnosis relies on clinical findings, echocardiography, and blood tests confirming prior streptococcal infection. Cardiac imaging helps assess valve damage and guides treatment decisions for both acute and chronic stages.
Treatment includes antibiotics to eradicate infection, anti-inflammatory medications, and in advanced stages, surgical valve repair or replacement. Preventive antibiotic therapy reduces recurrence and protects against further heart damage.
| Medical Term | Rheumatic Heart Disease |
| Definition | Chronic inflammatory condition that develops after acute rheumatic fever, usually involving the heart valves |
| Main Cause | Group A beta hemolytic streptococcal infection (usually after a throat infection) |
| Affected Structures | Most commonly mitral valve – less frequently aortic, tricuspid and pulmonary valves |
| Symptoms (Acute Phase) | Fever, joint pain, chest pain, shortness of breath, fatigue, skin rashes, chorea |
| Symptoms (Chronic Stage) | Shortness of breath, palpitations, exercise intolerance due to heart valve insufficiency or stenosis |
| Diagnostic Methods | Echocardiography, ECG, throat culture, ASO (antistreptolysin O) titer, Jones criteria |
| Treatment Methods | Antibiotics (penicillin), anti-inflammatory therapy (aspirin, corticosteroids), heart failure treatment, valve surgery in advanced stages |
| Prevention Methods | Early treatment of streptococcal infections, secondary prophylaxis (long-term penicillin injections) |
| Complications | Valve diseases, heart failure, atrial fibrillation, stroke risk |
| Follow-up Process | Regular cardiologic control, monitoring of valve function with echocardiography |
What is heart rheumatism and how does it start?
Rheumatism of the heart should not be thought of as a problem of the heart itself. It is actually the result of an abnormal reaction of the body. It all starts with a throat infection (pharyngitis) caused by a bacterium called group A streptococcus, commonly known as the “beta germ”. This is a feverish and painful throat infection that most of us had as children. If this infection is not treated with the right antibiotics and in sufficient time, our immune system experiences a kind of “identity confusion”.
The defense cells it produces to fight the bacteria begin to perceive our own heart valve tissues, which are structurally very similar to bacterial proteins, as “foreign” and “hostile”. As a result of this tragic misunderstanding, our defense system attacks not only the bacteria but also our healthy heart valves. This attack triggers a widespread inflammatory attack throughout the body called “acute rheumatic fever” (ARF for short). The permanent damage to our heart valves caused by these attacks, namely thickening, hardening and dysfunction of the valves, is called “rheumatism of the heart”. Unfortunately, this damage is permanent and gradually progresses over the years, disrupting the heart’s working patterns.
Why Acute Rheumatic Fever is an Alarm for Heart Rheumatism
Acute rheumatic fever (ARF) is the precursor and first step to rheumatism of the heart. This inflammatory reaction, which occurs about 2 to 5 weeks after an untreated throat infection, is the most important warning signal that carries the risk of permanent damage to the heart. Most of the symptoms known as signs of rheumatism of the heart, especially in children, actually occur during this ARA attack. These important clues, which are also referred to as “symptoms of rheumatism hitting the heart”, should be taken seriously.
The most common warning signs of acute rheumatic fever are:
- Fire
- Wandering joint pain and swelling (arthritis)
- Chest pain
- Shortness of breath
- Palpitations
- Involuntary muscle movements (chorea)
- Ring-shaped rashes on the skin
- Painless swellings under the skin
The appearance of any of these symptoms, especially in a child or young person who has recently had a sore throat, is a critical warning that a doctor should be consulted immediately to stop the development of rheumatism of the heart. While problems in the joints or skin usually heal without scarring, inflammation in the heart, or “carditis”, can cause permanent damage to the valves.
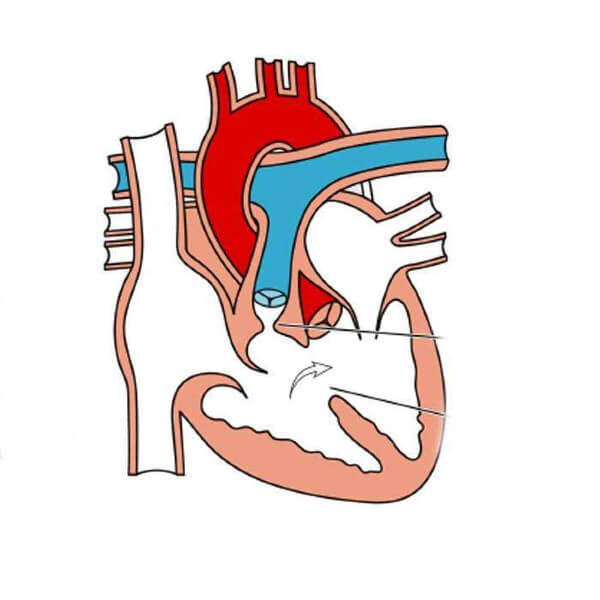
How Does Heart Rheumatism Damage the Heart?
The damage to the heart caused by rheumatism is not an instantaneous event; it is a slow, silent process that takes years. The body’s immune system attacks the heart valves, causing repeated attacks of inflammation. Each attack triggers a kind of wound healing process in the valves, but this healing is not normal healing. The constant cycle of wounding and repair leads to the formation of scar tissue (fibrosis) in the valves, i.e. thickening and hardening of the tissue.
During this process, the flexible leaflets of the heart valves gradually thicken, shrink and may stick together. Even the thin tendons (chordae tendinea) that hold the valves together like the strings of a parachute become shorter and stiffer. This damage, accumulated over the years, causes the valve to experience one of its two main dysfunctions.
- Valve Stenosis (Stenosis): The valve becomes so stiff and stuck that it cannot open to allow blood to pass freely. The heart has to work much harder to get the blood through this narrow gap.
- Valve Failure (Leakage): The valve becomes so deformed that it cannot close after pumping blood forward. Therefore, some of the pumped blood leaks backwards. This puts extra strain on the heart.
This damage most commonly affects the mitral valve on the left side of the heart, followed by the aortic valve.
What Symptoms Does Advanced Heart Rheumatism Cause?
One of the most misleading aspects of rheumatism of the heart is that the disease can progress silently for many years without any symptoms. Damage to the heart valves can begin soon after an attack of acute rheumatic fever, but thanks to the heart’s capacity to tolerate this damage, it can often take 10, 20 or even 30 years before obvious symptoms appear. Rheumatism of the heart in adults is therefore usually diagnosed when the heart can no longer carry the load.
The main symptoms that occur when damage to the heart valves becomes serious and starts to affect the pumping power of the heart are:
- Shortness of breath (especially with exertion or when lying down at night)
- Rapid fatigue and weakness
- Chest pain or feeling of pressure
- Swelling in the ankles, legs or abdomen (edema)
- Irregular heartbeat or a strong pounding sensation (palpitations)
- Dizziness or fainting
- Dry, persistent cough
The “murmur” heard with a stethoscope during a medical examination is the most important physical sign of valvular heart rheumatism and is often the first clue.
Who is more at risk for heart rheumatism?
Heart rheumatism is considered a “social disease” because its development is directly linked to living conditions. Although anyone can get this disease, some groups are at a significantly higher risk.
Risk factors include:
- children aged 5-15 years (the most at-risk age group for acute rheumatic fever)
- Poverty and malnutrition
- Crowded living spaces (schools, barracks, houses with many people living in the same room)
- Limited access to clean water and health services
- Family history of heart rheumatism
While this disease has almost completely disappeared in Western countries thanks to improved living standards and easy access to antibiotics, unfortunately, it is still a major public health problem in developing geographies, including our country.
How is Heart Rheumatism Diagnosed?
The diagnosis of cardiac rheumatism is not based on a single test, but on a combination of the patient’s history, physical examination findings and the results of various tests. This process is akin to detective work.
The basic steps and tests used in the diagnostic process are as follows:
- Patient History: Complaints such as recent throat infection, fever and joint pain are questioned.
- Physical Examination: One of the most important steps is to listen to the heart with a stethoscope and look for a “murmur” sound.
- Blood Tests: Tests such as CRP and sedimentation (ESR), which show inflammation in the body, and the ASO test, which proves previous streptococcal infection, are requested.
- Throat Culture: A throat swab is taken if active infection is suspected.
- Electrocardiogram (ECG): Records the electrical activity of the heart and can show rhythm disturbances or enlargement of the heart chambers.
- Echocardiography (ECHO): This is the gold standard test for diagnosis. ECHO, an ultrasound of the heart, confirms the diagnosis by clearly showing thickening of the valves, stenosis, leakage and the pumping function of the heart.
Is Heart Rheumatism a Preventable Disease?
The answer to this question is a clear and unequivocal “Yes”. Rheumatism of the heart is one of the greatest tragedies of modern medicine because it is 100% preventable. There is only one reason why this disease is now almost non-existent in high-income countries: Throat infections caused by streptococcal bacteria are taken seriously and treated in a timely manner with simple antibiotics such as penicillin. any condition that is dismissed as a “simple sore throat”, not taken to the doctor or left untreated with antibiotics can actually be an invitation to heart rheumatism. The fact that this preventable disease remains a problem shows how vital health awareness and access to health services are.
What Can Be Done to Prevent the Development of Heart Rheumatism?
Strategies to prevent heart rheumatism are twofold: preventing the disease from ever occurring (primary prevention) and stopping its progression once it does occur (secondary prevention).
- Primary prevention: Its aim is to prevent the first attack of acute rheumatic fever. The method is to detect the streptococcal throat infection early and to follow the antibiotic treatment (usually penicillin) prescribed by the doctor for the full duration (usually 10 days).
- Secondary prevention: This applies to people who have already had an episode of acute rheumatic fever or have been diagnosed with rheumatism of the heart. The aim is to prevent a recurrence of the disease and worsening of the damage to the heart by getting a new strep throat. This is the most basic step in managing the disease. The most effective method is long-acting benzathine penicillin injections into the muscle every 3-4 weeks, commonly known as “cardiac rheumatism injections”. Depending on the patient’s condition, this preventive treatment can continue for years, sometimes even for life.
What Methods Are Used in the Treatment of Heart Rheumatism?
Once damage to the heart valves has occurred, the answer to the question “does rheumatism of the heart valves go away?” is unfortunately no. There is no “cure” that completely removes the scar tissue and deformation. From this point on, treatment focuses on managing the disease, slowing its progression, controlling symptoms and preventing dangerous complications.
The main approaches used in the management of cardiac rheumatism are:
- Secondary prevention: Continue regular penicillin injections to slow the progression of the disease.
- Drug Treatment: Various medications are used to manage problems such as heart failure and arrhythmia.
- Interventional Methods: In appropriate cases of stenosis, a balloon can be used to dilate the valve (balloon valvuloplasty) in an angioplasty-like procedure.
- Surgical Treatment: In advanced cases, when medication and other methods fail, surgery is needed to repair or replace the damaged valve.
The medicines used are usually aimed at relieving the symptoms of heart failure. These include diuretics (diuretics), beta-blockers and ACE inhibitors to reduce the load on the heart, drugs to control arrhythmias and blood thinners (anticoagulants) to prevent the risk of clots.
Is Rheumatism of the Heart Dangerous and What Complications Does It Cause?
Yes, the answer to the question “Is rheumatism of the heart dangerous?” is definitely yes. It can lead to very serious life-threatening consequences, especially if left untreated or not followed up. Therefore, the question “can rheumatism of the heart kill?” can unfortunately also be answered yes. Progression of the disease can lead to serious complications, such as
Heart Failure: It is the most common and most important outcome.
Stroke (Paralysis): It usually occurs when a clot formed due to arrhythmia travels to the brain.
Atrial Fibrillation: It is a serious rhythm disorder that increases the risk of stroke by 5 times.
Infective Endocarditis: This is when the damaged valve becomes infected and can be fatal.
Pulmonary Hypertension: It is an increase in pressure in the lung vessels to dangerous levels.
These complications are the clearest indication of why the disease needs to be taken seriously and requires lifelong follow-up.
When is surgery for rheumatism of the heart necessary?
Determining the right time for heart valve surgery is one of the most vital decisions for the success of the treatment. The main goal is to intervene before irreversible muscle damage occurs in the heart. Rushing or delaying the decision to operate can have a negative impact on the outcome. Generally, surgery is considered when a patient starts to experience symptoms, or when there is objective evidence from tests such as echocardiography that the heart is becoming fatigued (reduced pumping power, enlargement of the heart chambers, etc.) even in the absence of symptoms. Waiting for symptoms can lead to permanent weakening of the heart muscle and incomplete recovery after surgery. The timing is therefore determined by careful consideration of the individual patient’s condition and the test results by a “Heart Team”.
What is the Difference Between Valve Repair and Replacement in Heart Rheumatism Surgery?
When the decision to operate is made, the most important question for the surgeon to answer is: “Can this cover be repaired or should it be replaced?”
Valve Repair: The aim of this procedure is to preserve the patient’s own natural valve. The surgeon makes your own valve functional again by opening adhesions, repairing tears and supporting the valve with a ring. Whenever possible, repair is always the first choice. This is because the long-term results are better, the risk of infection and clots is lower and, most importantly, there is usually no need for lifelong blood thinners. However, because rheumatic valves can be very hard and calcareous, their repair is technically difficult and not always possible.
Valve Replacement: If the valve is damaged beyond repair, the surgeon will completely remove the diseased valve and replace it with an artificial (prosthetic) valve. This is a definitive solution when repair is not possible, but it brings with it a new lifestyle and some of the obligations of a prosthetic valve.
How to Choose Mechanical and Biological Valves in Heart Rheumatism Surgery?
When the decision for valve replacement is made, another important decision that the patient and surgeon must make together is which type of prosthetic valve to use. There are two main options:
Mechanical Covers:
- They are made of very durable carbon materials.
- Their biggest advantage is that they last a lifetime.
- The biggest disadvantage is the need for lifelong use of blood thinners (Coumadin/warfarin) against the risk of clots.
Biological (Tissue) Caps:
- They are usually made from bovine or porcine heart tissue.
- Their biggest advantage is that they usually do not require blood thinners.
- Their biggest disadvantage is that they wear out over time (10-15 years on average) and require reoperation.
This choice is based on the patient’s age, lifestyle, pregnancy plan and personal preferences. Generally, mechanical valves are preferred in younger patients under 65 years of age and biological valves are preferred in older patients or patients who cannot use blood thinners.
What should be considered in rheumatism of the heart during pregnancy?
Cardiac rheumatism during pregnancy is a condition that requires special attention and very close monitoring. During pregnancy, the volume of blood in the body almost doubles. While a healthy heart can easily handle this load, a damaged valve may not be able to withstand this additional load and the mother may develop sudden heart failure. For this reason, it is vital for the health of both mother and baby that a woman with cardiac rheumatism is evaluated by a cardiologist before becoming pregnant, the risks are determined and the pregnancy process is followed up together by an experienced cardiologist and obstetrician.
What Should People with Heart Rheumatism Pay Attention to in Daily Life?
Heart rheumatism is a lifelong companion. In order to continue this journey in a healthy and quality way, the answer to the question of what to pay attention to those with heart rheumatism is very important.
Here are the most important points to consider to maintain your quality of life:
- Never miss your medical check-ups.
- Get your preventive penicillin injections (prophylaxis) regularly.
- Take your medicines (especially blood thinners) as prescribed by your doctor.
- Pay close attention to your dental health and hygiene.
- Always consult your cardiologist before tooth extraction or any surgical procedure.
- Listen to your body; contact your doctor immediately in case of new symptoms such as shortness of breath or swelling.
- Reduce salt consumption.
- Avoid smoking and alcohol.
- Lead an active life as much as your doctor allows.
Frequently Asked Questions
What is rheumatism of the heart?
It is a heart disease that develops after rheumatic fever, usually after a throat infection, when the immune system damages the heart tissue.
After which disease does it develop?
It occurs after a throat infection (tonsillitis) caused by beta-hemolytic streptococcus bacteria.
Which parts of the heart are affected?
The heart valves are most commonly affected. The mitral valve is the most commonly involved valve.
Who is more common?
It is common in children and young adults, especially in low socioeconomic areas.
What are the symptoms?
Pain in the joints, fever, chest pain, palpitations, shortness of breath and fatigue may occur.
How is it diagnosed?
Diagnosis is based on blood tests, throat culture, echocardiography and physical examination.
Is treatment possible?
Yes, treatment with antibiotics, anti-inflammatory drugs and long-term prophylaxis is possible.
Is this disease permanent?
It can cause permanent damage to the heart valves, in which case the disease becomes chronic.
Does rheumatism of the heart affect other organs?
Yes, joints, brain, skin and heart can be affected at the same time.
How is heart valve damage treated?
Severe valve disorders may require surgical valve repair or replacement.
Is rheumatism of the heart contagious?
No, the disease itself is not contagious, but the streptococcal infection is.
Is there a risk of recurrence?
Yes, new infections can trigger the disease again, which is why long-term antibiotic protection is needed.
What are the prevention methods?
Early diagnosis and treatment of throat infections and compliance with hygiene rules are the most effective ways of prevention.
Is heart rheumatism risky during pregnancy?
Pregnant women with valvular disease are at increased risk of complications; regular cardiology follow-up is essential.

Prof. Dr. Yavuz Beşoğul graduated from Erciyes University Faculty of Medicine in 1989 and completed his specialization in Cardiovascular Surgery in 1996. Between 1997 and 2012, he served at Eskişehir Osmangazi University Faculty of Medicine as Assistant Professor, Associate Professor, and Professor, respectively. Prof. Dr. Beşoğul, one of the pioneers of minimally invasive cardiovascular surgery in Türkiye, has specialized in closed-heart surgeries, underarm heart valve surgery, beating-heart bypass, and peripheral vascular surgery. He worked at Florence Nightingale Kızıltoprak Hospital between 2012–2014, Medicana Çamlıca Hospital between 2014–2017, and İstinye University (Medical Park) Hospital between 2017–2023. With over 100 publications and one book chapter, Prof. Dr. Beşoğul has contributed significantly to the medical literature and is known for his minimally invasive approaches that prioritize patient safety and rapid recovery.