Barlow syndrome, also known as mitral valve prolapse, is a valvular heart condition where the mitral valve leaflets bulge back into the left atrium during systole. It is usually benign but may sometimes lead to regurgitation, arrhythmias, or rarely, sudden cardiac events.
Clinical symptoms of Barlow syndrome include palpitations, chest discomfort, dizziness, and fatigue. Many patients remain asymptomatic, and the condition is often detected incidentally during echocardiographic examinations.
Complications associated with mitral valve prolapse include progressive mitral regurgitation, atrial fibrillation, and endocarditis. Regular monitoring with echocardiography helps in assessing valve function and preventing adverse outcomes.
Management strategies range from conservative observation to surgical repair or replacement of the valve in advanced cases. Lifestyle modifications, avoidance of stimulants, and medical therapy may be advised depending on symptom severity and progression.
| Definition | A clinical syndrome characterized by mitral valve prolapse (MVP), characterized by excessive movement of the valve leaflets into the left atrium, usually associated with myxomatous degeneration |
| Causing Factors | Genetic predisposition (autosomal dominant inheritance), connective tissue diseases (Marfan, Ehlers-Danlos), idiopathic myxomatous changes |
| Risk Factors | Family history, connective tissue diseases, female gender, development of myxomatous degeneration at advanced age |
| Symptoms | Chest pain, palpitations, syncope or presyncope, shortness of breath, anxiety, fatigue; some cases may be asymptomatic |
| Diagnostic Methods | Mid-systolic click and late systolic murmur on physical examination; transthoracic echocardiography (TTE), transesophageal echocardiography (TEE), ECG, Holter monitoring |
| Complications | Mitral regurgitation, risk of endocarditis, atrial fibrillation, ventricular arrhythmia, rarely sudden cardiac death |
| Treatment Methods | Asymptomatic cases are usually followed up; beta blockers, antiarrhythmics, surgery in severe mitral regurgitation (mitral valve repair or replacement) in symptomatic patients |
| Follow-up and Monitoring | Monitoring valve function and mitral regurgitation level with regular ECHO; ECG and Holter for arrhythmia monitoring |
| Ways of Prevention | No specific preventive methods; regular cardiologic follow-up and arrhythmia-oriented measures are recommended |
What is Barlow Syndrome and how does it differ from Mitral Valve Prolapse?
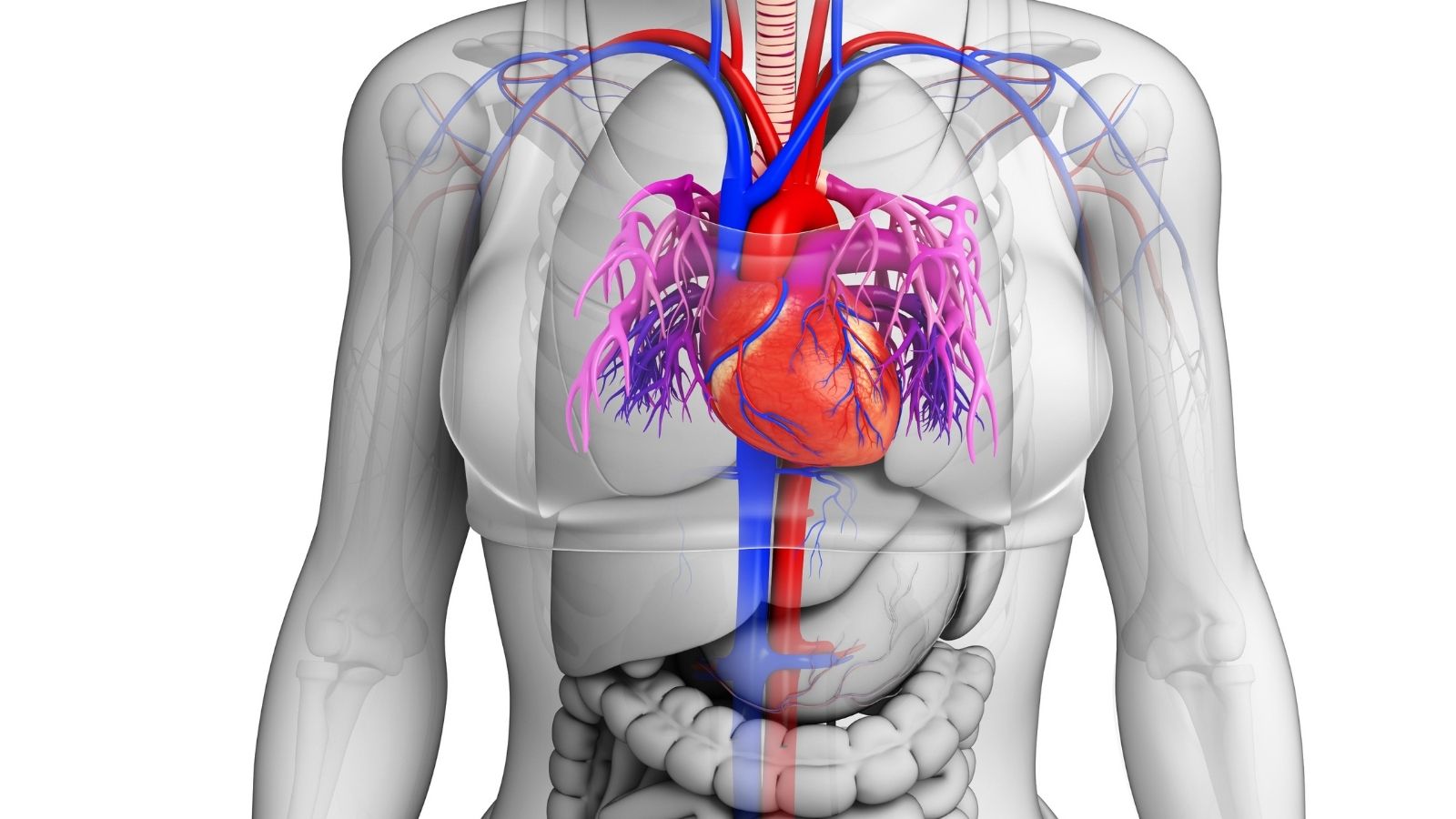
Inside our heart, there are four valves that work like a door, keeping the blood flowing in the right direction. The mitral valve is an important structure located between the left atrium and the left ventricle of the heart. When we say Barlow’s syndrome, we mean that the tissue of this mitral valve is thicker, more flexible and almost “loose” than normal.
Each time the heart contracts, it creates pressure to pump blood around the body. Normally, the mitral valve closes tightly against this pressure. However, in Barlow’s syndrome, these thickened and inflexible valves cannot withstand the pressure and bulge or sag slightly backwards, towards the left atrium. This general sagging condition is called mitral valve prolapse (MVP). Barlow syndrome is a special form of this condition in which the valve tissue is more prominent, bulkier and often more complex.
In short, every Barlow syndrome is a mitral valve prolapse, but not every mitral valve prolapse may involve a structural defect as severe as Barlow syndrome. Making this distinction correctly is critical for determining the follow-up and treatment strategy.
Who has Barlow Syndrome and how common is it?
Mitral valve prolapse and its variant Barlow syndrome are not uncommon in the general population. According to modern studies, it is estimated that between 1% and 3% of the general population has the condition. This means it affects millions of people worldwide.
Although the disease can occur at any age, even in infants, the classic diagnosis of Barlow syndrome is usually made in young adults under the age of 60, and often under the age of 40. Although it seems to be more common in women when first diagnosed, when the condition progresses and major problems such as serious valve leakage occur, it is observed that it becomes more predominant in men over the age of 50.
Genetic predisposition also plays an important role in Barlow syndrome. A family history of mitral valve prolapse is a factor that can increase the risk. Barlow syndrome may also be more common in people with genetic diseases that affect the body’s general connective tissue, such as Marfan syndrome or Ehlers-Danlos syndrome.
What changes does Barlow Syndrome cause in the heart valve?
The underlying process of Barlow syndrome is a tissue deterioration known in medicine as “myxomatous degeneration”. We can think of this as a change in the quality of the material that makes up the structure of the valve over time. A healthy valve has a balanced structure of both flexible and strong fibers, whereas in Barlow syndrome this balance is disturbed.
This process results in some typical changes in the valve and surrounding structures:
- Thickening and increased volume of valve tissue
- Formation of a spongy and loose structure
- Abnormal enlargement of the valve area (redundancy)
- Elongation and thickening of the strands holding the valve (chordae tendinea)
- Sometimes these strands stick together
- Enlargement of the ring (annulus) where the valve sits
- Separation of the valve ring from the heart muscle (mitral annular dysjunction)
What are the symptoms of Barlow Syndrome?
A significant proportion of people with Barlow syndrome may go for years without experiencing any symptoms. In many people, the diagnosis is made incidentally during a routine medical examination for another reason, when a murmur or “clicking” sound is heard in the heart.
However, when symptoms do occur, they are usually non-specific and vary from person to person. The most common symptoms of mitral valve prolapse are
- Palpitations A feeling that the heart beats irregularly, rapidly or with a misfire.
- Atypical Chest Pain: A pain that is usually sharp, stabbing and not directly related to exertion.
- Shortness of Breath: A feeling of breathlessness, especially during exertion or when lying on your back.
- Fatigue: Feeling tired more quickly than usual and low energy.
- Dizziness: Occasional feeling of lightheadedness.
- Anxiety and Panic Attacks: In some patients, mitral valve prolapse can trigger panic attack-like states.
Which methods are used to diagnose Barlow Syndrome?
Confirming the diagnosis of Barlow syndrome is like putting the pieces of a puzzle together. The process starts with listening to the patient’s story, continues with physical examination and is clarified with imaging methods.
- Patient History and Physical Examination: The first step is to listen carefully to your complaints and family history. Then the doctor listens to your heart with a stethoscope. The “mid-systolic click” (the clicking sound made by a valve that begins to sag) and the subsequent “late systolic murmur” (the blowing sound made by blood escaping backwards), which are characteristic of Barlow syndrome, are important findings that strengthen the suspicion.
- Imaging Tests: Various tests are used to confirm the suspicion on physical examination and to understand the severity of the condition. The main methods used in the diagnosis of Barlow syndrome are as follows:
- Echocardiography (ECHO): It is an ultrasound of the heart and is the gold standard of diagnosis. It clearly shows the structure of the valves, their thickness, the amount of prolapse and the degree of blood leakage.
- Electrocardiogram (ECG): Records the electrical activity of the heart and detects rhythm disturbances or wave changes that may indicate risk.
- Holter Monitor: records ECGs for 24 hours or longer, catching rhythm disturbances that go unnoticed during the day.
- Cardiac Magnetic Resonance (CMR): It is an advanced imaging technique that is invaluable in showing whether there is scar tissue (fibrosis) in the heart muscle that may predispose to rhythm disturbances.
Why is echocardiography so important in the diagnosis of Barlow Syndrome?
Echocardiography (ECHO) is an indispensable tool in the diagnosis of Barlow syndrome because it provides live moving images of the heart and valves. This allows us to see not only whether there is a “sagging” but also the anatomical details underlying this sagging.
Different types of ECHO provide different levels of information:
- Transthoracic ECHO (TTE): This is the standard test performed through the chest wall. It is usually sufficient to make the diagnosis and initial assessment. It measures clear criteria such as valves prolapsed more than 2 mm and thicker than 5 mm.
- Transesophageal ECHO (TEE): It is performed by inserting a thin probe into the esophagus. Since it is closer to the heart, it provides much clearer and more detailed images of the mitral valve. It is especially used to map the valve anatomy in full detail before surgical planning.
- 3-Dimensional (3D) ECHO: This modern technology shows the valves as a three-dimensional structure rather than a two-dimensional picture. It allows the surgeon to clearly see where and how much the valve is sagging and the volume of the tissue before surgery, allowing the surgeon to rehearse an operation.
Is Barlow Syndrome a problem that progresses over time?
Yes, Barlow syndrome is not a static condition but a progressive disease that usually progresses slowly over time. Although many patients remain stable for years, the underlying tissue deterioration persists, which can lead to increased valve prolapse and associated blood leakage (mitral regurgitation).
This progression means an increased load on the heart. The heart has to work harder to compensate for the backflow of blood. Over time, this extra work causes the heart to become tired and enlarged. This brings with it the risk of some serious complications in later years:
- Heart failure
- Need for surgical intervention
- Rhythm disorders such as atrial fibrillation
It is therefore vital that a person diagnosed with Barlow syndrome, even if they have no complaints, is under regular cardiologic follow-up to detect this progression early and intervene in time if necessary.
Is there a risk of sudden death in people with Barlow Syndrome?
This is one of the most sensitive and important questions on the minds of many people who receive this diagnosis. First of all, it is important to be clear: For the vast majority of patients with Barlow syndrome, the risk of sudden death from mitral valve prolapse is extremely low and the condition usually has a benign course.
However, there is a very small subgroup of patients who have what we call “malignant” disease. In this group, severe structural defects in the valve cause constant mechanical stress on the heart muscle beneath it. Over time, this tension can lead to the formation of small scar tissues (fibrosis) in the heart muscle. These scar tissues can act as a kind of “short circuit” in the heart’s normal electrical system, triggering serious life-threatening arrhythmias.
Our task as physicians is to identify this high-risk group of patients at an early stage. For this, we carefully assess certain risk factors:
- Family history of sudden death
- Unexplained fainting (syncope) episodes
- Specific T-wave changes on ECG
- Frequent and complex rhythm disturbances detected on Holter monitoring (PVC)
- Marked prolapse and thickening of both valves on echocardiography
- Detection of fibrosis in the heart muscle on cardiac MRI
Patients with one or more of these factors require closer follow-up and a proactive treatment approach.
When should a patient with Barlow Syndrome have surgery?
In Barlow syndrome, the decision to operate is made proactively before permanent damage to the heart occurs, rather than waiting until the symptoms are no longer tolerable. The aim is to preserve the health of the heart and enable the patient to maintain a normal life expectancy.
Surgical intervention usually becomes necessary in the following cases.
- Onset of Symptoms: If a patient with a serious valve leak develops complaints such as shortness of breath and fatigue, this is a clear reason for surgery.
- Impaired Heart Function: Even if the patient feels well, a decrease in the contractile force of the heart (ejection fraction – EF) below ` on ECHO is a sign that the heart is getting tired.
- Enlargement of the heart chambers: If the diameter of the left ventricle of the heart increases above a certain level (usually 40 mm) on ECHO, this indicates that the heart is permanently enlarged in response to the increased load.
- New Onset Rhythm Disorders: Especially the development of atrial fibrillation is an important warning.
- Increased Pulmonary Pressure: Another reason for surgery is that the valve leak increases the pressure in the pulmonary vessels (pulmonary hypertension).
Why is valve repair preferred over valve replacement in the treatment of Barlow Syndrome?
In the surgical treatment of degenerative valve diseases such as Barlow syndrome, repairing the patient’s own valve is far superior to replacing it with an artificial valve (replacement) whenever possible. Mitral valve repair is therefore considered the “gold standard” treatment.
There are very strong reasons behind this superiority of valve repair.
- Better Long-Term Survival: Studies show that patients with valve repair have a higher life expectancy than those with valve replacement, approaching that of their healthy peers.
- Preservation of Heart Function: Preserving the patient’s own valve and underlying support tissues better preserves the heart’s natural geometry and pumping function.
- No Need for Blood Thinners: Mechanical artificial valves require lifelong use of blood thinners (such as Coumadin). These drugs carry a risk of bleeding and affect quality of life. Valve repair saves patients from this necessity.
- Lower Risk of Infection and Clots: The risk of complications such as infection and clotting is much lower with repaired natural valves compared to artificial valves.
- Excellent Durability: Today’s modern repair techniques are so advanced that a repair carried out by experienced centers can last for decades.
Can Barlow Syndrome surgery be performed with a small incision (minimally invasive)?
Yes, absolutely. Even the most complex mitral valve repairs, such as Barlow syndrome, can now be successfully performed by experienced surgeons using minimally invasive or robotic surgery. These modern approaches offer many important advantages for patients compared to traditional open heart surgery (a full-thickness cut across the breastbone).
In minimally invasive surgery, a small incision of about 4-6 cm is made under the right lower chest, between the ribs. The surgeon performs the operation with the help of special instruments and a high-resolution camera inserted through this small incision.
The main benefits of this method to the patient are as follows:
- Faster Recovery: Patients are usually back on their feet sooner and return to their normal activities sooner.
- Shorter Hospitalization: Hospital discharge time is significantly shorter.
- Less Pain: Since postoperative pain is less, the need for painkillers is reduced.
- Less Blood Loss: The need for blood transfusion is lower.
- Better Cosmetic Result: Instead of a large surgical scar, a small scar remains, which is more aesthetically acceptable.
What should patients with Barlow Syndrome pay attention to in daily life and nutrition?
Barlow syndrome management is not just about medical treatments. Healthy lifestyle habits support your overall heart health and help reduce the risk of complications.
Generally recommended lifestyle changes include the following:
- Heart-Friendly Diet: Adopt a diet low in salt, saturated fats and processed sugars. Include plenty of vegetables, fruits, whole grains and lean protein sources such as fish.
- Weight Control: Being overweight increases the heart’s workload. It is important to maintain a healthy weight.
- Avoiding Tobacco: Smoking is the biggest enemy of cardiovascular health and should be quit.
- Stress Management: Chronic stress can trigger symptoms such as palpitations. It is beneficial to manage stress with methods such as meditation, yoga and regular exercise.
- Avoiding Stimulants: Especially if you suffer from palpitations, limiting or completely quitting caffeine (coffee, tea, energy drinks) and alcohol consumption may alleviate your symptoms.
- Oral and Dental Health: Regular dental check-ups and good oral hygiene are more important than you think for reducing the risk of valve infection (endocarditis).
Can a person with Barlow Syndrome exercise?
Exercise is an important part of Barlow syndrome management, but there is no “one-size-fits-all” prescription. The type and intensity of exercise should be determined according to the individual’s risk profile and the severity of the valve leak.
Low Risk Patients: Most patients who are not at risk of serious valve leakage, symptoms or arrhythmias can exercise with almost no restrictions, including competitive sports.
High Risk Patients: Patients with severe valve leakage or malignant phenotype features (history of fainting, severe arrhythmias, etc.) should avoid high-intensity and straining sports. This can increase the risk by raising blood pressure suddenly.
Types of exercise that are considered safe for most patients:
- Walking
- Swimming
- Yoga
- Light brisk cycling
- Resistance training with light weights
Before starting any exercise program, you should always consult with the cardiologist monitoring your condition to create the safest and most beneficial exercise plan for you.
Frequently Asked Questions
What is Barlow syndrome?
Barlow syndrome is a condition characterized by mitral valve prolapse (collapse), in which the mitral valve leaflets prolapse into the left atrium of the heart.
Is it the same as mitral valve prolapse?
Yes, Barlow syndrome is a form of mitral valve prolapse, especially the type where the leaflets are thick and redundant.
What are the symptoms?
Symptoms may include chest pain, palpitations, dizziness, fatigue, anxiety and shortness of breath.
Why does this syndrome occur?
It develops due to congenital weakness in the valve structure or connective tissue diseases.
Is it a dangerous disease?
In most cases it is mild and harmless, but in some patients it can lead to severe valve failure and rhythm disturbances.
How is Barlow syndrome diagnosed?
The most common diagnostic method is echocardiography; clicks can be heard on auscultation.
Does this syndrome cause heart failure?
If severe mitral regurgitation develops, there may be a risk of heart failure.
Is Barlow syndrome hereditary?
Yes, it can be familial; it is more common in individuals with connective tissue disorders.
Is there a cure?
Regular follow-up is sufficient in mild cases. If necessary, drug treatment and, in advanced cases, surgical intervention is applied.
Does Barlow syndrome require surgery?
If there is severe valve prolapse and insufficiency, mitral valve repair or replacement can be performed.
Is drug treatment effective?
Yes, medicines such as beta-blockers are used to relieve palpitations and chest pain.
Is it safe to exercise?
In mild cases, low-paced exercises are appropriate; if there are complaints, a doctor’s approval should be obtained.
Is Barlow syndrome progressive?
Some people may progress and develop valve insufficiency; regular follow-up is required.
Is there a risk of arrhythmia?
Yes, ventricular arrhythmias may occur in some cases; rarely there may be a risk of sudden death.
Who is at risk?
People who are tall, thin, with supple skin and those with a family history of connective tissue disease are more susceptible.

Prof. Dr. Yavuz Beşoğul graduated from Erciyes University Faculty of Medicine in 1989 and completed his specialization in Cardiovascular Surgery in 1996. Between 1997 and 2012, he served at Eskişehir Osmangazi University Faculty of Medicine as Assistant Professor, Associate Professor, and Professor, respectively. Prof. Dr. Beşoğul, one of the pioneers of minimally invasive cardiovascular surgery in Türkiye, has specialized in closed-heart surgeries, underarm heart valve surgery, beating-heart bypass, and peripheral vascular surgery. He worked at Florence Nightingale Kızıltoprak Hospital between 2012–2014, Medicana Çamlıca Hospital between 2014–2017, and İstinye University (Medical Park) Hospital between 2017–2023. With over 100 publications and one book chapter, Prof. Dr. Beşoğul has contributed significantly to the medical literature and is known for his minimally invasive approaches that prioritize patient safety and rapid recovery.