Leg pain occurs due to circulatory disorders, musculoskeletal problems, or nerve compression. Vascular causes such as varicose veins, deep vein thrombosis, or arterial occlusion are particularly important as they may indicate serious health risks. Early diagnosis prevents progression.
Leg pain treatment options vary according to the underlying cause. In vascular-related conditions, lifestyle adjustments, compression stockings, and medical therapies may be applied. For musculoskeletal issues, physical therapy and exercise programs are effective. Proper evaluation is essential before treatment.
Leg pain symptoms related to vascular insufficiency often increase during walking or standing and improve with rest. Sudden swelling, redness, or severe pain may indicate urgent problems such as thrombosis. Timely medical intervention significantly reduces complications and improves quality of life.
Preventive measures for leg pain include regular exercise, maintaining ideal body weight, and avoiding prolonged sitting or standing. Adequate hydration, a balanced diet, and quitting smoking support vascular health. Periodic check-ups are especially crucial for individuals with a family history of vascular disease.
| Definition | Formation of a blood clot in veins (veins) |
| Causes | Prolonged immobility, surgical operations, trauma, pregnancy, cancer, certain medications (especially birth control pills), genetic clotting disorders |
| Risk Factors | Age, family history of venous thrombosis, obesity, pregnancy, hormonal treatments, immobilization, cancer, varicose veins, heart failure |
| Symptoms | Aching, pain, tenderness, redness, redness, heat increase, may be asymptomatic depending on the location of the occluded vein |
| Diagnostic Methods | Doppler ultrasonography, D-dimer test, venography, CT or MR-angiography |
| Treatment Methods | Anticoagulant drugs (blood thinners), thrombolytic therapy, compression stockings, rarely surgical intervention |
| Complications | Pulmonary embolism, postthrombotic syndrome, chronic venous insufficiency |
| Prevention Methods | Early mobilization, compression stockings, anticoagulant prophylaxis, increased fluid intake, avoidance of risk factors |
What is Venous Thrombosis and Why Should It Be Taken Seriously?
When you hear the term venous thrombosis, you need to understand that there are actually two important interrelated conditions. These conditions are like different stages of the disease and together they are called venous thromboembolism.
The first condition is known as Deep Vein Thrombosis (DVT). This is when the clot forms in large veins, usually deep in the legs, hidden between muscles. This clot in the leg vein blocks the blood’s route back to the heart like a roadblock. As a result, blood begins to pool behind the clot, increasing the pressure inside the vein and causing symptoms such as aching, pain and warmth in the leg. DVT in itself is an uncomfortable condition that requires treatment.
But the most dangerous side of venous thrombosis occurs when this clot or a fragment of it dislodges. This clot fragment that gets caught in the bloodstream is called an embolus. This stray clot embarks on a journey through the bloodstream, passing through the right side of the heart and eventually reaching the arteries of the lungs that allow us to breathe in and out. This clogging of the lung vessels is called Pulmonary Embolism (PE), or clot in the lung as it is commonly known. This is an extremely serious and life-threatening condition that requires urgent intervention. The sudden interruption of blood flow to the lungs prevents oxygen intake and can lead to sudden shortness of breath, chest pain and, unfortunately, even sudden death. Therefore, DVT should not just be seen as a leg problem, but should be taken seriously as a potential harbinger of a pulmonary embolism.
Which Risk Factors Increase the Danger of Venous Thrombosis?
Venous thrombosis is rarely caused by a single cause. It is usually caused by the accumulation of multiple risk factors over time, like a glass gradually filling up. Thrombosis occurs when the threshold for a person to form a clot is exceeded by a combination of these factors. Venous thrombosis risk factors are conditions that predispose to clot formation. These factors act by slowing blood flow, damaging the vessel wall or making the blood itself more prone to clotting.
The main factors that increase the risk of venous thrombosis are:
- Major surgical operations (especially hip, knee, abdominal and cancer surgeries)
- Serious accidents, trauma or bone fractures
- Prolonged bed rest
- Immobility due to conditions such as paralysis
- Active cancer disease
- Chemotherapy or radiotherapy treatments
- Pregnancy and the first six weeks after delivery (puerperium)
- Use of birth control pills or hormone replacement therapy
- Older age (risk increases with age)
- Obesity (being overweight)
- Smoking
- Presence of heirs
- History of previous DVT or pulmonary embolism
- Inherited clotting disorders (Thrombophilia)
- Heart failure or chronic lung disease
- Inflammatory bowel diseases (Crohn’s, Ulcerative Colitis)
- Long journeys (over 4 hours) by plane, bus or car
- The presence of devices such as intravenous catheters or pacemakers in the body
Among the factors on this list, “Thrombophilia”, or hereditary clotting disorders, is a condition in which a person’s blood is genetically predisposed to clotting. This may be suspected in people with a family history of clotting at a young age. However, genetic predisposition alone does not necessarily mean that a person will develop clots. Usually, the risk of thrombosis increases significantly when an additional risk factor such as a long journey, surgery or pregnancy is added to this genetic background. It is therefore important to think of risk factors as links in a chain and to recognize that the more links that connect, the greater the risk.
What are the Symptoms of Deep Vein Thrombosis and Pulmonary Embolism?
The symptoms of venous thrombosis can vary completely depending on where the clot is located. Sometimes, especially with small clots, it may not cause any symptoms at all and may be detected incidentally during tests for another reason. But when they do appear, it is vital to recognize these signals and take them seriously.
Common symptoms of a clot in the leg (Deep Vein Thrombosis – DVT) are the following:
- Pain, which usually occurs in one leg (visible difference in diameter between the two legs)
- Pain, cramping or tenderness in the calf or thigh
- Significant temperature increase in the affected leg compared to the other
- Skin discoloration such as redness, bruising or pallor
- Superficial veins become more prominent and fuller than normal
- Increased pain, especially when walking or standing
Symptoms that occur in the event of a clot in the lung (Pulmonary Embolism – PE) and require urgent intervention include the following:
- Sudden and unexplained shortness of breath
- Sharp chest pain that intensifies when breathing deeply, coughing or bending over
- Persistent cough, usually dry but sometimes accompanied by bloody sputum
- The heart beats much faster and louder than normal (palpitations)
- Severe dizziness, lightheadedness or sudden fainting
- Excessive sweating and cold, damp skin
- A feeling of intense anxiety or fear of death
If any of these symptoms occur, especially if they follow signs of DVT, this can be a strong sign that the clot has reached the lung. Suspicion of a pulmonary embolism is a medical emergency where even seconds count and professional help should be sought immediately by calling 112 or contacting the emergency department of the nearest hospital.
What Methods Are Used to Diagnose Venous Thrombosis?
When a patient’s complaints raise suspicion of venous thrombosis, the diagnostic process proceeds in careful and systematic steps. The aim is both to confirm the diagnosis and to avoid unnecessary tests. This process is based on the doctor confirming or denying clinical suspicion through a series of tests.
The first step is always to listen to the patient’s detailed history and perform a thorough physical examination. The doctor will ask when and how the patient’s symptoms started, whether there are any other accompanying symptoms and which of the risk factors listed above the patient has. Information such as whether he or she has recently traveled a long distance, had surgery, or has a family history is invaluable. In the physical examination, the difference in weight between the legs is measured, discoloration and tenderness are checked. From this initial assessment, the doctor mathematically estimates the likelihood of a clot as low, medium or high using special clinical scoring systems (such as the Wells or Geneva score). This likelihood score plays a critical role in determining what to do next.
The main diagnostic tools used after the probability assessment are:
D-dimer Blood Test: When a clot forms in the body and the body’s natural defense mechanisms try to break it up, a protein particle called D-dimer is released into the blood. This test measures the level of this particle in the blood. The most important feature of the D-dimer test is that it can rule out venous thrombosis with a high degree of confidence (above one) in patients with a low or intermediate likelihood of clots, when the result is negative. So if the D-dimer is normal in a low-risk patient, no further testing is usually necessary. However, a high D-dimer level alone does not necessarily mean that there is a clot. Many other conditions such as pregnancy, infection, cancer, trauma or old age can also raise the level. A high D-dimer is an alarm bell and sends the message “we need to dig deeper with imaging tests”.
Color Doppler Ultrasonography: It is the first choice and most reliable imaging method for the diagnosis of deep vein thrombosis. This test uses sound waves to show the internal structure of the veins and blood flow in real time. It is completely painless, harmless and radiation-free. During the test, the specialist gently presses on the leg veins with the probe of the ultrasound device. A healthy vein is easily crushed under this pressure and its walls press together. However, a vein with a clot in it resists this pressure and does not close because it is like a pipe full of blood. This finding of “no compression” is the surest sign for the diagnosis of DVT. In addition, the presence, direction and speed of blood flow within the vessel can also be assessed thanks to the color Doppler feature.
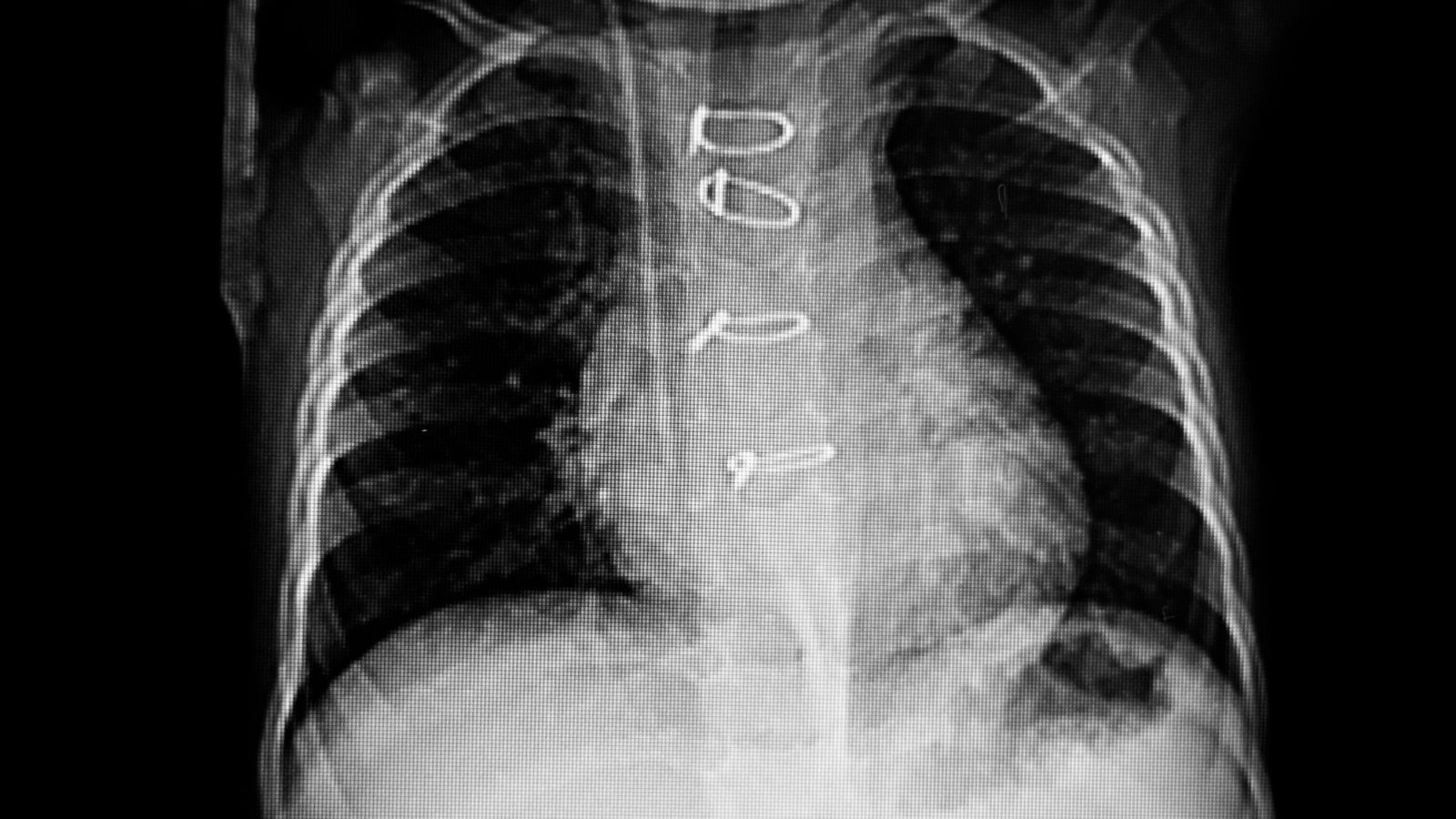
Computed Tomography (CT) Pulmonary Angiography: The gold standard diagnostic method for detecting a clot in the lung (pulmonary embolism). For this test, an iodinated contrast agent (dyed medicine) is injected into a vein in the patient’s arm. As it travels rapidly through the bloodstream into the lung arteries, the CT scanner takes cross-sectional images of the lungs. The contrast medium shows the vessels in a bright white color. If there is a clot in the vessel, it blocks the passage of the contrast medium and is clearly visible as a dark “filling defect” in the vessel. In addition to showing the location and size of the clot, CT angiography has the advantage of detecting other lung and heart problems that can cause shortness of breath, such as pneumonia or a ruptured aorta.
What are the Current Venous Embolism and Thrombosis Treatment Options?
The treatment of venous thrombosis has been revolutionized in recent years. Whereas in the past the options were more limited, today we are able to create individualized, much more effective and safer treatment plans based on the patient’s condition, the size of the clot and the risk it poses. Our main goals in treatment are to prevent the clot from growing and spreading to the lungs, to prevent the formation of new clots and, most importantly, to preserve the patient’s long-term quality of life by minimizing the permanent damage that the clot will leave in the vessels.
Blood Thinners (Anticoagulant Therapy)
This treatment is the mainstay of venous thrombosis management and is given to almost all patients. It is important to know that contrary to popular belief, these drugs do not directly “dissolve” the existing clot. Blood thinners prevent the clot from growing larger and new clots from being added. This gives the body’s own natural clot-dissolving system (fibrinolytic system) time to gradually clear the existing clot.
Traditional Approach (Warfarin/Coumadin): For many years, standard treatment consisted of heparin-type injections started in hospital, followed by oral warfarin medication at home. Although warfarin is an effective drug, it had many challenges, such as it was difficult to find the right dose, its effect varied with many foods (especially green vegetables) and drugs, and it required constant blood tests (INR monitoring) to check its effect.
Next Generation Oral Anticoagulants (DOACs): These drugs, which have been gaining ground in treatment over the last decade, have largely overcome the difficulties of conventional therapy. They provide great comfort for both patient and physician, as they are used in fixed doses, do not require routine blood monitoring and have far fewer food interactions. Large scientific studies involving tens of thousands of patients have shown that this new generation of drugs is at least as effective as warfarin and significantly reduces the risk of the most feared side effect, cerebral hemorrhage. For these reasons, they have become the first choice for the treatment of venous embolism and thrombosis in most patients today.
Interventional Therapies (Clot Dissolution and Removal)
In some cases, especially in the case of large clots that extend from the groin to the abdomen and cause severe pain, soreness and bruising in the leg (large iliofemoral DVT) or a large life-threatening pulmonary embolism, simply giving a blood thinner is not enough. In these cases, our goal is more proactive: To actively remove the clot blocking the vessel. This is where modern endovascular methods applied by cardiovascular surgeons come into play, which are performed by entering through the vein without making large incisions in the body.
Catheter-directed thrombolysis: In this method, a thin needle is inserted through a vein, usually behind the knee, in the angiography laboratory. Through this needle, a special catheter (thin plastic tube) with many small holes in it that allow the drug to be pushed through is advanced up to the heart of the clot. Through this catheter, clot-dissolving multi-power drugs (such as tPA) are slowly and directly into the clot over many hours. This targeted treatment prevents the drug from spreading throughout the body, reducing the risk of systemic bleeding and ensuring maximum effect on the clot.
Mechanical Thrombectomy (Physical Removal of the Clot): With the advancement of technology, sophisticated devices have been developed that physically shatter, suck or both the clot instead of just dissolving it with drugs. These methods are a lifesaver, especially for patients for whom the use of clot-dissolving drugs is risky. These devices can shatter the clot in the vein with a high-speed rotating wire, dissolve it with sound waves (ultrasound) or, with the most modern approach, aspiration thrombectomy, suck the clot out of the body like a powerful vacuum. These methods, which allow the vein to be cleaned only by vacuum, especially without the use of clot-dissolving drugs, can be safely applied even in patients at high risk of bleeding (for example, those who have recently undergone major surgery or have stomach bleeding) and open a new frontier in treatment. By opening the vessel quickly, these interventional treatments both relieve symptoms in the acute phase and significantly reduce the risk of developing permanent damage to the leg (Post-Thrombotic Syndrome).
What Complications Can Occur in the Long Term After Venous Thrombosis?
Even after the acute danger of venous thrombosis has been overcome, unfortunately for some patients it may not end there. The clot can leave permanent damage to the vessel wall and in particular to the delicate valves that prevent blood from backing up. This damage leads to chronic problems that build up over the years and seriously affect a person’s quality of life.
Post-Thrombotic Syndrome (PTS): The most common long-term complication, occurring in approximately 1 to P of patients with deep vein thrombosis, especially those with a large clot to begin with. The clot destroys the valves in the vessel, which function like a one-way valve. When these valves break down, blood cannot be pumped to the heart effectively against gravity and the legs begin to constantly tear. This condition is called chronic venous hypertension and causes a range of unpleasant symptoms.
Chronic complaints caused by post-thrombotic syndrome include the following:
- Chronic pain, heaviness and fatigue in the leg that does not go away or increases throughout the day
- Stubborn pain (edema), which is especially pronounced in the evening and is difficult to relieve with rest
- Discoloration of the skin, especially around the ankle, in the form of brown-red spots
- Hardening, thickening and loss of elasticity of the skin (lipodermatosclerosis)
- Severe itching and eczema-like rashes
- In the most advanced stage, painful sores (venous ulcers) that are easily opened even with minor trauma and can take months or even years to heal
PTS is a condition that can severely limit a patient’s daily activities, work and social life. Therefore, treating DVT effectively at the onset, especially with interventional methods aimed at completely opening the vein, is the most important step in preventing the development of PTS.
Chronic Thromboembolic Pulmonary Hypertension (CTEPH): In a small percentage (0.5 – 4%) of patients with pulmonary embolism, the clots in the lung vessels cannot be completely cleared by the body. Over time, instead of dissolving, these clots organize, harden and adhere to the vessel wall, turning into scar tissue. These persistent clogs create a serious resistance to blood flow in the lung arteries, which can cause lung pressure to rise to dangerous levels. This rare but very serious condition is called CTEPH. It leads to progressive shortness of breath, fatigue and eventually right heart failure. The most important and promising feature of CTEPH is that, unlike many other types of pulmonary hypertension, it is potentially completely curable with surgery. In this highly specialized and complex open-heart surgery called Pulmonary Thromboendarterectomy (PTE), the surgeon opens the lung arteries and carefully peels and removes this organized, chronic clot material like a membrane. A successful PTE surgery can completely open the patient’s lung vessels, restoring blood flow to normal and completely curing the patient of this serious disease. For this reason, it is vital that patients with persistent shortness of breath after a pulmonary embolism be evaluated in a specialist center in this respect.
What Are the Ways to Prevent Venous Thrombosis While Hospitalized?
A significant proportion of all cases of venous thrombosis develop during hospitalization or after major surgery. Immobility, the surgery itself and the underlying disease create a perfect storm environment for clot formation. Therefore, assessing the risk of clots in almost every hospitalized patient and taking preventive measures (prophylaxis) to reduce this risk is a standard of patient safety in modern medicine.
The main methods used in hospitals to prevent clots from forming are the following:
Low Dose Blood Thinners Drugs: Patients at risk are given low-dose heparin injections, usually under the skin of the abdomen, to reduce the tendency of blood to clot. In some cases, low-dose oral blood thinners can also be used.
Compression (Varicose Veins) Stockings: These special stockings apply decreasing pressure on the leg from the ankle upwards, preventing blood from stagnating in the deep veins and accelerating the flow of blood to the heart.
Intermittent Pneumatic Compression Devices: Used as an additional measure, especially in high-risk (e.g., neurosurgical patients) or very high-risk patients for whom the use of blood thinners is risky. These devices massage the leg muscles and mechanically support blood circulation by raising and lowering the manones wrapped around the patient’s legs at regular intervals.
Early Action (Mobilization): Perhaps one of the simplest but most effective methods. Sitting on the edge of the bed, standing up and walking in the corridors as soon as possible after surgery activates the muscle pump, stimulates blood circulation and naturally reduces the risk of clots.

Prof. Dr. Yavuz Beşoğul graduated from Erciyes University Faculty of Medicine in 1989 and completed his specialization in Cardiovascular Surgery in 1996. Between 1997 and 2012, he served at Eskişehir Osmangazi University Faculty of Medicine as Assistant Professor, Associate Professor, and Professor, respectively. Prof. Dr. Beşoğul, one of the pioneers of minimally invasive cardiovascular surgery in Türkiye, has specialized in closed-heart surgeries, underarm heart valve surgery, beating-heart bypass, and peripheral vascular surgery. He worked at Florence Nightingale Kızıltoprak Hospital between 2012–2014, Medicana Çamlıca Hospital between 2014–2017, and İstinye University (Medical Park) Hospital between 2017–2023. With over 100 publications and one book chapter, Prof. Dr. Beşoğul has contributed significantly to the medical literature and is known for his minimally invasive approaches that prioritize patient safety and rapid recovery.